- A subarachnoid haemorrhage is bleeding into the space between the pia and arachnoid mater which usually contains the circle of Willis and its major branches.
- Blood tends to track into Sulci and ventricles and basal cisterns.
- Any new severe headache with onset to maximum severity within 2 minutes lasting for at least 60 minutes should be treated as a possible SAH.
- 50% of patients die within 48 hours irrespective of therapy.
- Patients with aSAH usually go straight from the emergency department to the Neurosurgeons/Neurointensive care for coiling or clipping.
- Stroke physician or neurologist may be involved if a no aneurysm is found usually after formal angiography has been carried out.
- Some may develop stroke due to vasospasm and are referred back for post stroke rehabilitation.
- The stroke physician must be comfortable with and understand the basics and theory behind SAH and its causes and management.
incidence
- There are about 6 cases per 100 000 patient years and most patients are < 60 years of age.
- 1-2% of population have an unruptured aneurysm.
Causes
| Cause | Comments |
|---|
| Aneurysmal | SAH due to a saccular/berry aneurysm rupture causes 85% of cases |
| Non Aneurysmal Perimesencephalic | This may be diffuse or just see some blood in front of the pons. Causes 10%. Seen mostly in middle age 50+ . The headache may be less acute. Loss of consciousness and syncope are exceptional. | |
| Traumatic | mild to moderate head injury often in elderly |
| Intracranial Dissection | Dissection commoner in carotid but vertebral artery dissections are more likely to cause SAH. May see lower cranial nerve palsies and lateral medullary syndrome. |
| Arteriovenous malformations | rare to bleed only into subarachnoid space only and there is usually a intraparenchymal haematoma. Aneurysms can form on the feeding arteries of an AVM and these are more likely to bleed than the AVM. | |
| Dural Arteriovenous malformations | usually affect the tentorium and resembles aSAH. |
| RCVS | Thunderclap headache middle aged female and convexity SAH |
| Amyloid angiopathy | Older person and convexity SAH |
| Others | Neoplasms, dural AVM, venous angiomas, infectious aneurysm |
| Vasculitis | Rare |
Imaging
Berry/Saccular aneurysms
Berry aneurysms cause the vast majority of spontaneous SAH. However most saccular aneurysms will never rupture. Any aneurysm can rupture, although statistically larger (>1cm - 4%) aneurysms are more likely to do so. However smaller aneurysms are common so most bleeds are from small aneurysms between 5-10 mm, when they rupture. It is commoner in Women than Men and incidence and increases linearly with age. The old theory that it was due to a structural defect due to absent media has been refuted. Saccular aneurysms are never seen in neonates and rarely in childhood and are so developmental and enlarge through life. About 10-15% of patients presenting with SAH
have multiple aneurysms. There appears to be an increased risk with smoking and hypertension both of which are treatable.
Non-aneurysmal non traumatic SAH
Occasionally the SAH is not due to an aneurysm but then a search must go on to try and determine its source. Head trauma is a cause but these patients usually go initially under trauma teams or neurosurgeons. If there is no aneurysm or AVM or other macrovascular anomaly then there is little for the surgeons to do acutely other than manage any hydrocephalus or clot evacuation. These patients may have angiography early and with no cause found and may end up then under the care of the stroke team.
Causes may include
- Peri mesencephalic SAH where often no cause found and possible venous bleed
- Amyloid angiopathy and a bleed from a vessel usually on the convexity of the brain in the elderly
- RCVS: usually a bleed from a vessel usually on the convexity of the brain associated with thunderclap headache in middle aged women
- Anticoagulants and mild or unrecalled trauma can exacerbate any cause
|
The main message is that unless there are other confounding comorbidities that these patients usually have a good prognosis. The prognosis for the peri mesencephalic variety is usually excellent.
Commonest sites of intracranial aneurysms
- (a) posterior inferior cerebellar artery
- (b) basilar artery tip 5%
- (d) internal carotid artery (ICA) and Pcomm 35%
- (e) anterior communicating artery (ACA) 35%
- (f) bifurcation of the middle cerebral artery (MCA) 20%
|
Risks
- Smoking, Binge drinking, Illicit drugs
- No real evidence for role for hypertension
- Adult polycystic kidney disease
- Marfan's/Ehlers Danlos syndromes
- Pseudoxanthoma elasticum
- SLE and Sickle cell
|
Clinical
- Worst ever headache comes on over seconds to maximal within 5 minutes
- Severe "hit round back of head with a shovel"
- Comes on at rest, sleep, coitus and straining
- May be associated with episode of collapse and then recovery
- Headache may be back of head and cervical in some cases
- Photophobia and meningism
- Coma and coning and sudden death
- Some claim warning headaches over preceding weeks "herald bleeds"
- Fundoscopy - subhyaloid haemorrhage
- Headache + 3rd nerve palsy due to compression of the 3rd nerve by the PCommA. The pupil is dilated.
- Monocular blindness from an anterior communicating artery aneurysms if it is exceptionally large
| Complications of SAH | Comments |
|---|
| Vasospasm | May cause later cerebral infarction usually at 3-12 days. A large amount of subarachnoid blood on CT is a predictor of the development of vasospasm. Prevent with Nimodipine for 21 days, positive fluid balance, and prevention of hyponatraemia |
| Re bleeding | May be seen in 20% of patients in the first 2 weeks. Peak incidence of rebleeding occurs the day after SAH. This may be from lysis of the aneurysmal clot |
| Hydrocephalus | May develop the first day due to obstruction of CSF outflow in the ventricular system by clotted blood. Can occur early (EVD) or late (VP shunt). Careful with drainage as a sudden reduction in ICP can increase the risk of rebleeding. CT shows that temporal horns are dilated and there is diffuse SAH and blood in the 4th ventricle with diffuse cerebral oedema |
| Coning | Due to mass effect with fall in GCS and dilated pupil(s) |
| Epilepsy | Fall in GCS or seizure like movements |
| Hypothalamic dysfunction | Excess sympathetic stimulation, which may lead to myocardial ischaemia or labile BP |
| Hyponatraemia | May be due to renal salt wasting or due to SIADH |
| Nosocomial pneumonia | May be seen in ITU with fall in SaO2 and pyrexia and CXR changes |
Differential
- Venous sinus thrombosis
- Benign orgasmic cephalgia
- Migraine
- Primary intra Parenchymal haemorrhage
- Brain tumour with bleed
- Carotid/vertebral dissection
If 3rd generation CT negative < 6 hrs then SAH excluded. If done after 6 hrs must still do LP at 12 hrs to look for xanthochromia
Investigations
- Bloods: FBC, U&E, LFTs may detect hyponatraemia
- ECG: 20% have ECG evidence of myocardial ischaemia and ST segment elevation, T wave changes due to high levels of circulating catecholamine. Measure troponin if concerned
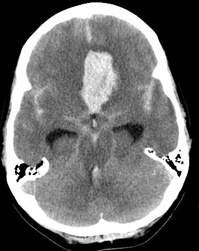
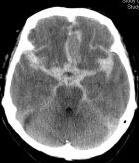
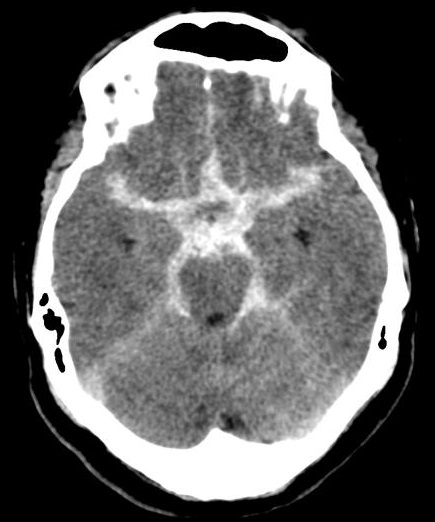
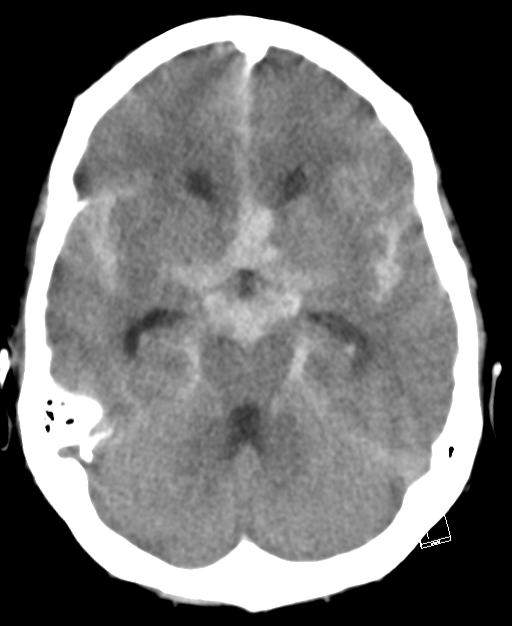
- CT head: With modern scanners CT scan is almost 99% sensitive in the first 6 hrs and then 90% sensitive within the first 24 hours, 80% sensitive at 3 days, and 50% sensitive at 1 week. There is high signal attenuation in the basal cisterns, Sylvian fissure, or intra hemispheric fissure. CT higher concentrations of blood over the convexities or within the superficial parenchyma of the brain are more consistent with the rupture of an AVM or a mycotic aneurysm. A CT can detect hydrocephalus. With perimesencephalic SAH the main haemorrhage is located anterior to the brainstem and is less likely to cause hydrocephalus with enlargement of the temporal horns.
- Lumbar Puncture: If CT is negative but the history convincing then LP is done at 6-12 hours after onset. Blood in itself is not diagnostic as even the smoothest puncture can hit a vein. What is needed is evidence of blood breakdown products suggesting a bleed over 6-12 hours ago. A RBC < 2000 x 106 and negative and negative xanthochromia excludes SAH. Xanthochromia (which measures bilirubin by photo spectrometry) is still present up to 2 weeks. False negative with severe anaemia or small-volume SAH. Xanthochromia is a classic sign, but not present early - look for equal or increasing blood in the sample tubes or D-dimer
- Catheter angiography (DSA) for detecting aneurysms is being replaced by CTA. If bleeding is identified then Cerebral angiography is the definitive study to identify the source of subarachnoid haemorrhage but CTA generally being used. If multiple aneurysms are found treatment targeted towards aneurysm adjacent to largest blood collection. Sometimes there may be significant difficulty identifying the source. Usually DSA is needed unless when there is clear evidence of a perimesecephalic SAH when CTA alone may suffice.
- Transcranial doppler can detect vasospasm of the MCA
| World federation of Neurological Surgery Grades |
|---|
- I. GCS 15 No focal deficits
- II. GCS 13-14 No focal deficits
- III. GCS 13-14 focal deficits present
- IV. GCS 7-12 irrespective of deficits
- V. GCS 3-6 irrespective of deficits
|
| Hunt and Hess Grades |
|---|
- 0: Unruptured aneurysm
- 1:Asymptomatic or min headache & without neck rigidity
- 2:Moderate-severe headache, neck rigidity and cranial nerve palsy
- 3:Drowsy, confused, mild focal deficit
- 4:Stupor, mild-severe deficit, decerebrate rigidity
- 5:Deep coma, decerebrate, moribund
|
Management
- Acute:ABC, Referral to Neurosurgeons and/or Neuro-intensive care depending on GCS and airway. Absolute bed rest, codeine for headache and laxative/stool softener.
- Medical Care:Hydration and slight hypervolaemia is suggested. Give 3 L of N-saline over 24 hours (unless poor cardiac function). Do not water restrict if hyponatraemia as more likely due to renal salt loss.
- Vasospasm prevention:In those with suspected aneurysmal SAH Start Nimodipine 60 mg 4 hrly to reduce vasospasm for 21 days. Nimodipine has been shown to reduce neurological deficit, cerebral infarction and mortality.
- Aneurysm Management: Cerebral Angiography is performed and if an aneurysm is identified then patient is assessed for coiling or clipping of the aneurysm.
- Clipping: Neurosurgical aneurysm clipping requires a craniotomy, performed under general anaesthesia. It takes 4-8 hours and has a procedural mortality rate of 1-3%. Early clipping - less rebleeding but higher incidence of vasospasm. Worst time is day 7 to 10 (highest time for vasospasm) So < 3 days or > 10 days. Notably Coils are not MRI compatible and is avoided. CT will also show lots of artefact.
- Coiling: Endovascular obliteration by means of detachable platinum spirals (coiling) is the preferred mode of treatment. They were first used in 1991. Coils when unwound can be between 1 to 60 cm long. Soft metal coils also absorb some of the pulse pressure of normal blood flow. It is a minimally invasive percutaneous endovascular treatment, which has proved to be a safe alternative to traditional surgical clipping of the aneurysm and may be associated with a better outcome in selected patients. The technique consists of packing the aneurysm with multiple detachable coils and is performed under general anaesthesia. It avoids craniotomy, and recovery after the procedure is more rapid. It is not indicated in 5-15% of cases, due to morphological or positional aneurysm characteristics. Performed by neurosurgeon or interventional neuroradiologist. Notably Coils are usually MRI compatible. CT will show lots of artefact so MRI preferred.
- Clipping vs Coiling: International Subarachnoid Aneurysm Trial (ISAT) Lancet 2002. 2143 patients randomized to NS clipping (n=1070) or endovascular coiling (n=1073). Outcomes at 2 months and 1 year. Better outcome with coiling with 23.7% vs 30.6% dependent or dead at 1y (ARR 7% NNT 14)
| Clipping requires craniotomy | Coiling can be done by catheter |
|---|
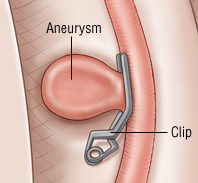 | 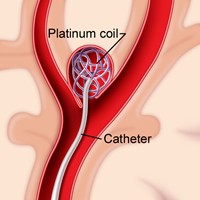 |
Management of Vasospasm
The triple H refers to hypertension, hypervolaemia, and haemodilution. Increase blood pressure to offset loss of autoregulation and hydrate to reduce blood viscosity which may reverse vasospasm. Target SBP 120-150mmHg in untreated aneurysms and up to 200mmHg in aneurysms that have been clipped or coiled. Early clipping or coiling, within 72 hours, is now the goal for all grades of SAH. It is an accepted technique, despite being unproven. Risks are volume overload and cardiac failure with myocardial ischaemia, and concerns it may provoke rebleed especially in those with unclipped aneurysms. Also Target Haemodilution Hct 30-35%
Further reading and references