Learning objectives
|
Introduction
The standard definition for stroke was of a neurological deficit of presumed vascular origin lasting for greater than 24 hours. This is very similar to the WHO diagnosis shown below. The presumed vascular origin was on the basis that this definition preceded widespread access to brain imaging. Widespread access to CT scanning was only available outside of the teaching hospitals really in the late 80s and even then CT scanning was often delayed and often not done at all. A time limit of 24 hours was also used based on the arbitrary length of a day which has little to do with brain vascular pathophysiology. However transient neurology has quite a different differential to persisting neurology so a minimum time limit would make the diagnosis more specific. In reality stroke is simply brain damage due to a local vascular cause such as the occlusion or rupture of a blood vessel. The World Health Organisation defines stroke as the sudden onset of focal neurological signs, of presumed vascular origin, lasting longer than 24 hours or causing death however many patients show brain damage on imaging well before 24 hrs and in reality we don't wait 24 hrs before labelling events as stroke when we are giving acute therapies.
Types of Stroke
Stroke is simply divided into Ischaemic Stroke and Haemorrhagic Stroke. Clinically this can be done as soon as a non-contrast CT has been done as the sensitivity for haemorrhage within the first 12 hours is over 99%. The vast majority of strokes are Ischaemic (80%) and a much smaller fraction are Haemorrhagic (15%). The remainder are Subarachnoid haemorrhages (5%). This varies and in those of Afro-Caribbean and Asian origin haemorrhagic strokes tend to be more common. With the wide availability of brain imaging Stroke is most simply divided by its CT acute appearance into Ischaemic and Haemorrhagic. Clinically this can be done as soon as a non-contrast CT has been done as the sensitivity for haemorrhage within the first 12 hours is over 99%.
| Ischaemic Stroke | Haemorrhagic Strokes | |
|---|---|---|
| Embolic/thrombotic/Low flow 80% | Intracerebral 15% | Subarachnoid 5% |
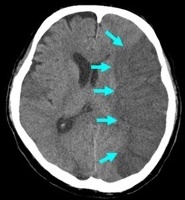 |  |  |
Strokes and some of their causes
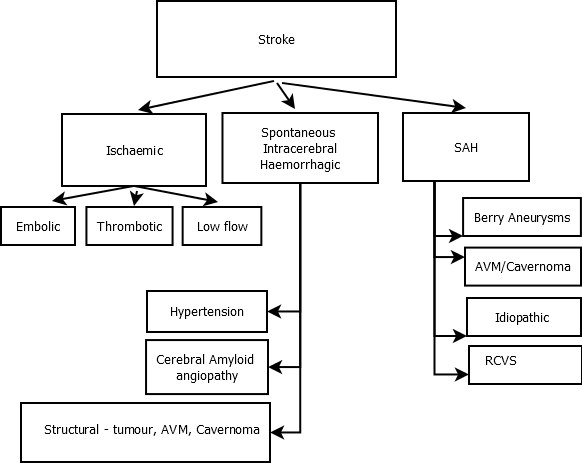
The vast majority of strokes are Ischaemic (80%) and a much smaller fraction are Haemorrhagic (15%). The remainder are subarachnoid haemorrhages (5%) This varies and in Asian countries for example haemorrhagic strokes tend to be slightly more common.
Bamford classification / Oxford Community Stroke Classification
There are many ways of classifying stroke. One commonly accepted method is the Oxford Stroke Classification, also known as the Bamford classification. The Bamford classification divides people with stroke into four different categories, according to the symptoms and signs with which they present. This classification is useful for understanding the likely underlying pathology, which in turn gives information on treatments likely to be useful and the prognosis. It is a relatively simple, robust, bedside classification using clinical information. A CT scan can be used to further classify the type of stroke into a bleed (intracranial haemorrhage) or infarction (thromboembolic) stroke. Clinical examination cannot do this reliably, so the CT scan is useful - but it does not make the diagnosis of stroke nor rule it out should the CT scan be normal.
- Lacunar infarcts (LACI): A pure motor stroke, a pure sensory stroke, a sensori-motor stroke, or an ataxic hemiparesis.
- Total anterior circulation infarcts (TACI): A combination of new higher cerebral dysfunction (e.g. dysphasia), homonymous visual field defect and ipsilateral motor and/or sensory deficit of at least two areas (out of face, arm and leg).
- Partial anterior circulation infarcts (PACI): Only two of the three components of a TACI, or with higher cerebral dysfunction alone, or with a motor/sensory deficit more restricted than those classified as LACI (e.g. confined to one limb).
- Posterior circulation infarcts (POCI): Any of: ipsilateral cranial nerve palsy with contralateral motor and/or sensory deficit; bilateral motor and/or sensory deficit; disorder of conjugate eye movement; cerebellar dysfunction; isolated homonymous visual ?eld defect.
TOAST Aetiological Classification
Stroke is a clinical syndrome that does not define causality. Once the stroke is diagnosed the search is on to find out why and there are more than 150 known causes. A simple form of classification is useful to help focus down on the possible causes and to help direct investigations and treatment. Strokes can broadly be divided using the TOAST criteria. This is derived from a trial of ORG 10172 in acute stroke treatment (TOAST) classification and denotes five sub types of ischaemic stroke. I have added estimated incidence and haemorrhage simply for clarity.
| Large-artery atherosclerosis (embolus / thrombosis)* | 20% |
| Cardioembolism (high-risk / medium-risk) | 20% |
| Small-vessel occlusion (lacune) | 20% |
| (Haemorrhagic) | 12% |
| Stroke of other determined aetiology | 5% |
| Stroke of undetermined aetiology | 30% |
It is thought to carry good inter observer agreement and predict prognosis, outcome, and management
Stroke Diagnosis
Stroke can be diagnosed in one of three ways - clinical, imaging and post-mortem. Imaging that can diagnose stroke has only be readily available for about 30 years and in the early days was often hard to access. The most common way is with simple history and examination and evidence of a persisting loss of function attributable to a specific and focal vascular event often corroborated with imaging lasting more than 24 hours. Up until now changes on imaging have not always been necessary to make a stroke diagnosis and if the clinical syndrome lasted more than 24 hours the label stroke was used. We often diagnose Ischaemic strokes by diagnosing the clinical syndrome of stroke and excluding haemorrhagic stroke acutely on CT. Further scanning such as MRI is done if the stroke location or diagnosis is uncertain. Ultimately the diagnosis of stroke depends on a Bayesian model of test + a priori risk.
| Modality | Comments |
|---|---|
| Clinical | A Clinical syndrome with a constellation of symptoms and signs attributable to a specific vascular occlusion can make a clinical diagnosis very accurate, For example a RSW + Dysphasia and RHH is classical for L MCA infarction even if the initial CT is normal as is often the case in a hyperacute scenario. However, a monoparesis e.g. hand or leg alone may warrant other tests to exclude a peripheral or other cause. A weak face alone may raise possibility of Bell's palsy. A weak hand with ipsilateral facial weakness is a much stronger sign of contralateral cerebral pathology and should be sought. Much of what we do is pattern matching to precise vascular territories. All ischaemic strokes are by and large arterial or penetrating arteriole or venous syndromes. |
| Imaging | Imaging has improved greatly. Back in the 1970s and before clinicians were using a calcified pineal and various equations and algorithms to locate a midline on plain X ray head as an identifier of midline shift and asymmetry and thereby an expanding haematoma or cerebral oedema. Now we have CT which is over 99% sensitive for bleeding. It will show infarction after 4-6 hrs but is notoriously unreliable for posterior fossa and small lesions. MRI is much more sensitive and is the diagnostic test of choice when there is any uncertainty. However for various reasons many cannot have MRI and so the diagnosis is based on clinical + CT which can leave some diagnostic uncertainty and where the diagnosis is unclear or uncertain the stroke physician has to hedge their diagnosis and treatments. |
| Post mortem | Pathological post mortem diagnosis is now much less common and although one can do a tissue diagnosis the act of cutting into brain distorts and disrupts the architecture and in many cases simple CT or even better MRI is more useful. Post mortem diagnosis was however the only sure way to diagnose stroke up until the era of modern imaging. Tissue however can be useful in identifying diseases such as amyloid angiopathy and some other diagnosis where tissue has particular diagnostic and microscopic and staining characteristics or even electron microscopy features. There has been a huge reduction in the number of PMs performed. |
MRI has moved the goalposts and we are now much clearer in diagnosing and identifying small strokes particularly sub cortically or in the brainstem and cerebellum. The guidelines from the US define a stroke based on evidence of radiological evidence of brain infarction. Haemorrhagic strokes are easily determined on non-contrast CT. However, the issue with an imaging based diagnosis is that not all patients will be able to have an MRI for logistical, practical and medical reasons. CT is not always conclusive and will miss small infarcts so we will still sometimes have to rely on clinical markers of brain injury and the presence of a persisting focal deficit.
I spend my days asking myself "is this stroke and if not what could it be". I take a history and examine. I look at the CT and assess a priori risk of stroke. If needed I can get an MRI. The more data I have allows me more certainty about the diagnosis. However acute therapies such as thrombolysis are done sometimes when there is some doubt as CT will be normal. As stroke physicians our experience and training gives us our own internal diagnostic threshold. In some centres MRI is done acutely but that isn't feasible in other centres. But there is some belief that some strokes can be MRI negative initially though that is controversial. To sum it all up ...
| Stroke Diagnostic threshold = Clinical evidence + Imaging evidence + "A priori" Stroke risk |
There are times when one just cannot be sure. Jane is a 52-year-old lady with a weak right arm and leg which came on acutely. Some aspects make you consider that it could be functional or even malingering. Jane refuses an MRI due to claustrophobia and CT is normal. Exam shows some give way weakness. Jane slowly improves to the point of discharge. However, Jane smokes and has hypertension which inflate her a priori stroke risk. You decide to give a statin, an antiplatelet and BP medications and encourage smoking cessation. You are left feeling uncertain about the diagnosis but feel on balance that the risk factors need management and she is labelled as a probable left Lacunar infarct. However, in a fit healthy 22-year-old with no vascular risk factors a non-vascular aetiology would be considered such as migraine or functional as the a priori risk is so small.
| Reasons why MRI not possible |
|---|
|
Transient Ischaemic attack
The diagnosis of TIA is so much more difficult and nuanced and much less accurate as CT/MRI imaging evidence by definition is negative and the clinical evidence is historical rather than real time and depends on recall by the patient and observer which can often be different. There is a much greater uncertainty. TIA historically has been defined as stroke like clinical syndrome which resolves within 24 hours and it is assumed that imaging shows no tissue evidence of infarction. However, with the sensitivity of MRI we can see small strokes whose symptoms resolve within hours. The pragmatic and practical approach is that if a patient tells you that they had a stroke-like episode and it resolves quickly then a TIA diagnosis may be reasonable. Don't however label a patient you actually see who has a deficit as a TIA even if symptoms fluctuate as any deficit that persists should be treated as stroke and discussed with stroke team. I think most of us would regard symptoms beyond 20 minutes from time of onset as an early stroke rather than a TIA and you should be considering urgent scanning and the need for reperfusion therapies.
The vital point is that a TIA or even a small transient stroke is a potential harbinger of further events and so should be assessed and managed quickly to look for modifiable risk factors. Prevention of further events is realistic and should be the primary focus. The role of a stroke physician includes secondary prevention, but the main stroke prevention physicians are the family physicians who manage stroke risk factors and prevent strokes from happening at all through health advice, treating hypertension and detecting and anticoagulating AF.
Terminology
Generally we avoid the term CVA and talking about 'accidents'. Stroke is a universally understood and preferred term. We should no more called strokes cerebrovascular accidents than we cause MI as cardiovascular accidents. Some prefer the more strident 'Brain attack'. Stroke does in itself produce a huge range of clinical severity from asymptomatic 'silent' disease found on imaging to patients who are moribund and die almost instantly due to massive brain infarction or haemorrhage. A pragmatic definition is a stroke is a clinical neurological deficit of presumed vascular origin lasting more than 24 hours or with evidence of brain infarction or haemorrhage seen on imaging or found at post-mortem.
Other terms you may see used
- Stroke in evolution: - Ongoing varying symptoms and signs over 24 hours, consider critical carotid artery stenosis (once haemorrhagic stroke excluded) or Capsular warning syndromes usually due to thrombotic strokes. The term overlaps with crescendo TIAs and depends on your choice of label.
- Reversible Ischaemic Neurological defect (RIND) - symptoms lasting for 24 hrs to 3 weeks. Used really premodern imaging. Adds little to understanding of stroke. An outdated historical term.
Patient and Stroke Selection
It is important that there is a clear destination for patients with stroke and those with associated non stroke conditions to avoid confusion and poor care.
| Type | Comments |
|---|---|
| Ischaemic | Stroke Team and stroke unit |
| Haemorrhagic | Neurosurgical consult if needed. Stroke Team and stroke unit |
| Thunderclap headache no neurology | Medical until CT/LP and then referral to Neurology/Neurosurgery/Stroke Physician as determined by likely diagnosis |
| Aneurysmal Subarachnoid | A stroke but usually goes to Neurosurgery for Coiling/clipping |
| Non-Aneurysmal Subarachnoid | Neurology/Stroke team for further investigations |
| Traumatic Subarachnoid | Not stroke. Trauma team/ Neurosurgery and head injury care |
| Subdural | Not stroke. These are extra axial. Trauma team/ Neurosurgery and head injury care |
| Extradural | Not stroke. These are extra axial. Trauma team/ Neurosurgery and head injury care |
Developments
Significant organisational and medical advances have occurred in the past 15 years. There has been a major change in the management of stroke patients, involving the transfer of care from general wards into dedicated multidisciplinary stroke units. The idea of specialized stroke units was first conceptualized in the 1980s, but only widely implemented after meta-analyses of multiple small trials showed that organized stroke care led to significant improvements in outcome, with a 20% reduction in both mortality alone (odds ratio (OR) 0.81) and the combined outcome of death and disability (OR 0.79) [3]. These improvements were observed both in a mixed population of strokes [1], and also in patients who presented with intracerebral haemorrhage [2]. Patients need to have immediate access to Hyperacute stroke units, Stroke Thrombolysis/thrombectomy and Neurosurgical access when appropriate. All those with strokes need to be on a dedicated stroke unit within 4 hrs of arrival at hospital and be looked after by a dedicated, educated, skilled team of doctors, nurses, therapists, therapy assistants, healthcare assistants. Stroke-unit care improves outcomes due to better prevention of complications. It is therefore important that all stroke patients, including the very old and frail, are admitted to specialist care as soon as possible. It is also a place where patient centred end of life care can happen if needed.
Secondly thrombolysis and more recently stroke thrombectomy has shown us that early directed therapies can reduce disability and the era of stroke medicine being a passive non interventional speciality has long gone. The first trial to demonstrate benefits of the National Institute of Neurological Diseases Stroke (NINDS) trial which came out in 1995. However the UK was slow to respond to the potential of stroke thrombolysis. For many years stroke care was patchy indeed. There has been huge catch up across the country and thrombolysis has been one of the drivers that has invigorated stroke medicine and stroke care has undoubtedly improved. The improvement has also been for those who didn't get thrombolysed but are assessed and admitted to a stroke unit along the same pathway. Much of this has been driven by the Sentinel Stroke work which became SSNAP coming out of the Royal College of Physicians. It is shocking to think that outside some pockets of excellence up until only 5-10 years ago many stroke patients were managed on general medical or elderly care wards and had very limited access to therapy and stroke specialist input. This hopefully is a thing of the past.
In this time there has been a greater interest in the evidence base for stroke and stroke research has really taken off outside the academic neuroscience centres. There is huge amounts of work to be done looking at all aspects of both Ischaemic and haemorrhagic stroke. The amount of money spent on research in stroke is small in comparison with other diseases such as breast cancer or heart disease or HIV. It is important to avoid the avoid the defeatist attitude of some towards stroke and focus on interventions that can really change the future of stroke medicine.
The future is about making sure that we do not loose these gains in the new austerity and making sure that reducing disability is good for patients but also for the taxpayer in terms of lifelong need for support. The future is also about increased research. An extension to the uses of thrombolysis, improved management of Hypertension and AF to reduce strokes as well as national strategies on smoking and obesity and exercise. The role and evidence base for Interventional neuroradiology continues to develop but the procedures are limited in availability to selected regional centres and even then on a very patchy basis. This hopefully will change with time and the encouragement of more staff to work in stroke.
References
- [1] Stroke Unit Trialists' Collaboration. Organised inpatient (stroke unit) care for stroke. Cochrane Database Syst. Rev. 2013
- [2]Langhorne, P.et al. on behalf of the Stroke Unit Trialists' Collaboration (2013). Stroke Unit Care Benefits Patients With Intracerebral Haemorrhage: Systematic Review and Meta-analysis. DOI: 10.1161/STROKEAHA.113.001564
- [3] Parr E et al. Management of Acute Stroke in the Older Person Geriatrics 2017, 2, 27; doi:10.3390/geriatrics2030027