Welcome
| Free Downloads |
|---|
| Latest Trial and other News |
|
New Focus Trial Collaboration results: "Fluoxetine 20 mg given daily for 6 months after an acute stroke does not seem to improve functional outcomes. Although the treatment reduced the occurrence of depression, it increased the frequency of bone fractures. These results do not support the routine use of fluoxetine either for the prevention of post-stroke depression or to promote recovery of function." Link to Lancet Full article 5th December 2018 ARISTOPHANES Study: In this largest observational study to date on NOACs and warfarin, the NOACs had lower rates of stroke/ Systemic emboli and variable comparative rates of Major Bleed versus warfarin. The findings from this study may help inform the discussion on benefit and risk in the shared decision-making process for stroke prevention between healthcare providers and nonvalvular atrial fibrillation patients Link to Stroke Article 8 Nov 2018 |
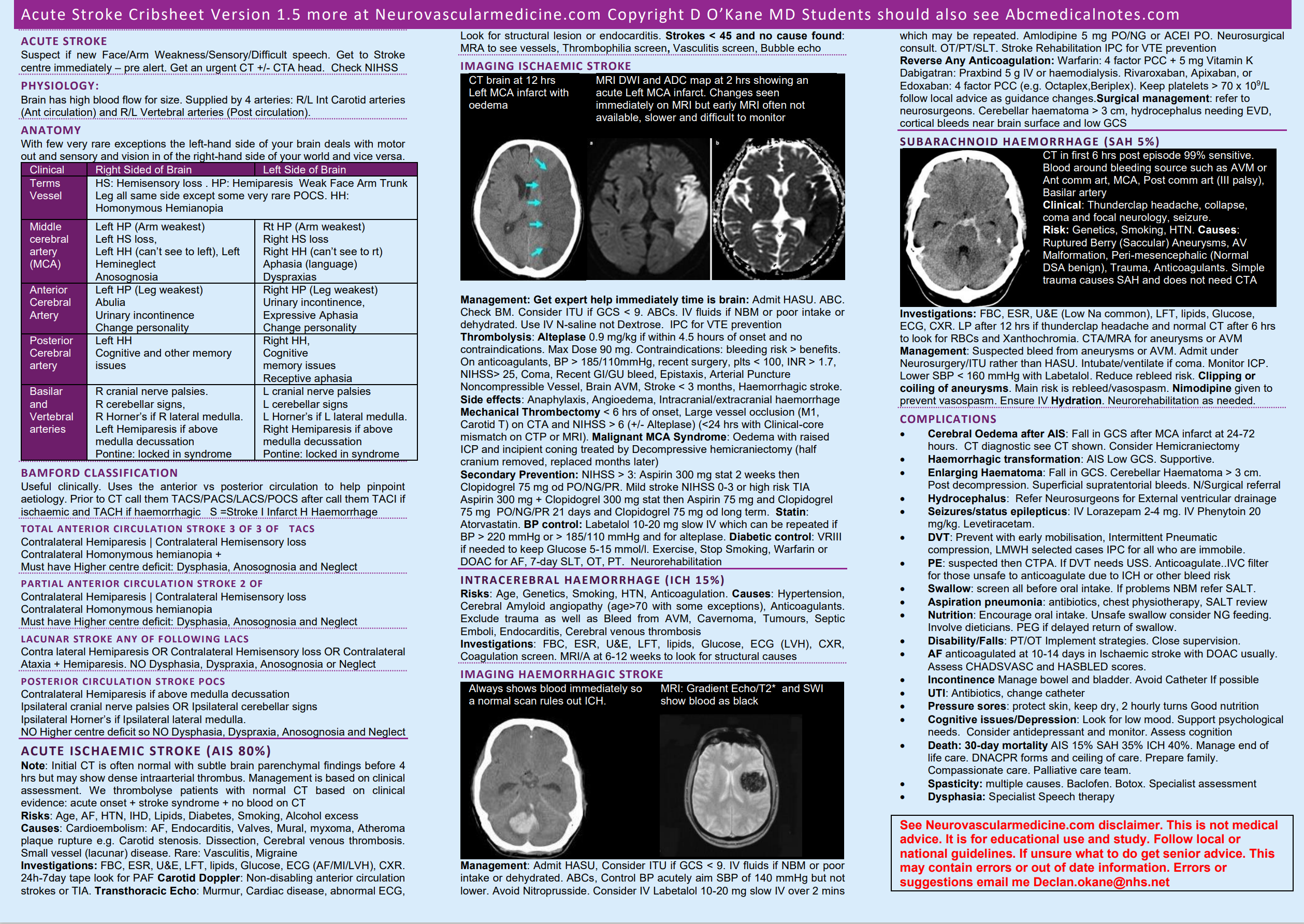 Stroke Crib Sheet
Stroke Crib SheetWelcome
Welcome to this website. This is a collection of short notes on many topics related to stroke medicine. Many topics are being added and updated and it is an ongoing process. It has been written primarily as a rich learning environment for students and trainees but is open for all who want to learn about stroke. Stroke medicine is a challenging and fascinating clinical speciality. You need to have a good understanding of Neuroscience and Neuroanatomy as well as Neuropathology, Neuroimaging as well as acute medicine, geriatric medicine, cardiology and respiratory and palliative medicine. You need to be able to manage complexity and apply logic and critical thinking in making the diagnosis and working out the cause or causes of the stroke as well as assessing risks and benefits of clinical interventions. Key skills also include team working with good communication, decision making and problem-solving skills. Much of our time is spent talking with patients, families, nurses, therapists and radiological, medical and surgical colleagues. As you will see we spend a lot of time doing medical detective work to discover why a stroke has happened as this allows us to try and prevent further strokes. Strokes can happen at all ages and we see several patients each year who are in the late teens or early 20s with stroke. We also spend our time in trying to prevent strokes and in those with modifiable risk factors. This is often done in the TIA clinic better called a stroke prevention clinic. Here we establish the diagnosis of TIA and screen and treat identifiable risk factors. Major risk factors include Atrial fibrillation and hypertension as well as many others.
Introduction
A Stroke is brain damage due to a localised vascular cause. This can be occlusion of a blood vessel due to a localized thrombus or embolism causing an Ischaemic Stroke or rupture of a blood vessel and bleeding into or over the surface of the brain which is called a Haemorrhagic Stroke. Stroke is very much about the large and small blood vessels that carry blood to and from the brain and how things can go wrong.
If you are the stroke physician on call you will be seeing a whole variety of patients where you rapidly need to triage with focused history taking, examination and imaging. It can feel like spinning plates constantly keeping a busy show on the road and you need to be skilful as well as knowledgeable and sensible. If you are interested in stroke medicine as a career then please talk to local specialists about doing a taster week or an elective or even a rotation. You will be welcomed. Stroke is challenging but fascinating. We are now in an era when we can do more than just diagnose and explain but we can actually make a dramatic difference to the outcome.
Stroke is common worldwide and the main risk factors are well known and many of the causes are preventable. Globally, however, stroke is the second most common cause of death in the world, causing around 6.7 million deaths each year. There are more than 100,000 strokes occurring in the UK each year which works out at one stroke every five minutes. There is some good news however, stroke incidence rates fell 19% from 1990 to 2010 in the UK. Despite my warning above stroke is predominately an issue for the over 60s. The average age for men and women to have a stroke is 74 and 80 respectively. However, a quarter of strokes happen in people of working age and one of the challenges is in supporting patients back to work. There are over 1.2 million stroke survivors in the UK.
Stroke care has changed massively in the past 10-20 years. Nowadays all stroke patients receive Hyperacute care and are admitted to a HASU (Hyperacute stroke unit) which was not always the case and have a chance to have access to proven evidence-based effective treatments such as thrombolysis, thrombectomy, neurosurgery when needed and multidisciplinary care and prevention of complications as well as stroke-specific rehabilitation. There has never been a better time to be involved in stroke care.
This is part of my work towards promoting free access to medical knowledge online also known as FOAMed. Please bookmark the page and share with colleagues and please come back again. I am chair of the Training and Education committee at British association of stroke physicians which I would recommend to any physicians working in the UK should join. This website does not reflect the views of BASP and only my own opinions.
Recent changes and developments are coming quickly and we all need to get on with delivering these. The next few years will see the development of thrombectomy services throughout the UK using different models. It is vital that we use all the tools available to improve prognosis and outcome from this disease which is so disabling to so many of our patients.
If you have any comments or would like to donate images or cases or any other teaching material then please contact me. I have based the content broadly on the Stroke and Vascular Fellowship curriculum. Stroke is constantly changing and will keep a record here of latest developments and interesting papers and references.