Learning objectives
- Learning
- Understand
- Integrate
- Reflect
|
Introduction
- MELAS is an acronym for Mitochondrial encephalomyopathy, lactic acidosis, and stroke-like episodes.
- It is a disorder of mitochondrial function and oxidative phosphorylation which affects organs with high metabolic needs (brain/muscles)
- The end result is ischaemic damage due to presumed transient oxidative phosphorylation dysfunction within the brain parenchyma.
Aetiology
- Mutations in a particular transfer RNA gene, MT-TL1, cause more than 80 percent of all cases of MELAS.
- Importantly they can occur de novo or be inherited maternally.
- Oxidative phosphorylation (or OXPHOS in short) is the metabolic pathway which is used to reform ATP.
- This takes place inside mitochondria. It is highly efficient way of producing ATP.
- A lack of ATP results in cell dysfunction and death "infarction" but without vessel obstruction
- Therefore it is "stroke like" but not stroke in the true sense
Clinical
- Onset is often in childhood with muscle weakness and pain.
- Patients may experience headaches, loss of appetite, vomiting, and seizures due to the lactic acidosis.
- Stroke-like episodes usually but not always before age 40
- Hemiparesis, coma, myoclonus, ataxia, hemianopia, seizures, and severe headaches resembling migraines.
- Relapsing-remitting course with an accumulation of injury leading to progressive brain damage with progressive disability
- Ongoing weakness, altered vision, cognition.
- Short stature and hearing loss which is sensorineural.
- Behavioural and psychiatric problems are noted.
- Schizophrenia has been diagnosed in some patients.
Diagnosis and related tests
- U&E,glucose: some develop Type 1/2 Diabetes
- ECG - a small number have HOCM, WPW and long QT syndromes
- Venous Blood Gas:Lactic acidosis may not cause a systemic metabolic acidosis
- Elevated serum lactate. Lactic acid concentrations measured after anaerobic exercise of the forearm.
- CSF lactate may be elevated even when serum lactate is normal. Elevated ratio between lactate and pyruvate is high.
- Skeletal muscle biopsy: classically Ragged red fibres in : morphological, biochemical, and molecular study of the muscle biopsy
- Genetic testing: identify gene mutations
- CT/MRI shows basal ganglia calcification - imaging discussed below
Investigations
- ABG: Arterial lactate and pyruvate are high
- CSF: Lactate also may be high. Lactate and pyruvate may increase substantially with exercise. Lactate/pyruvate ratio may be increased.
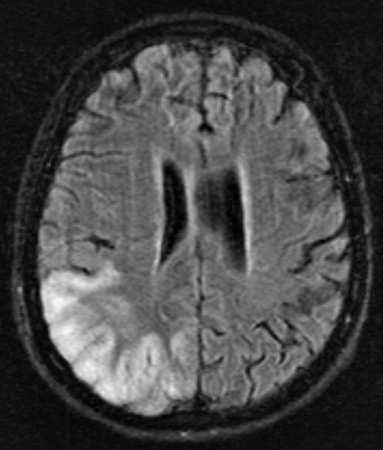
- CT/MRI: Acute infarcts acute infarcts will demonstrate swollen gyri with increased T2 signal. May enhance. Subcortical white matter involved. There may be T2 shine through on DWI with little change on ADC mapping (vasogenic not cytotoxic oedema). Multifocal stroke-like cortical lesions in different stages of evolution crossing the cerebral vascular territories. There is a predilection to the posterior parietal and occipital lobes. There is basal ganglia calcification more prominent feature in older patients. MR spectroscopy may demonstrate elevated lactate in otherwise normal appearing brain.
- Mitochondrial DNA analysis: 80% due to mutation is at position 3243 of the nucleotide sequence and 8% are at position 3271.
Management
- MELAS remains a largely untreatable condition. Manage acute medical complications may prolong survival.
- An accurate early diagnosis can help manage treatment
- Progress is usually inexorable but phenotypes can vary.
- Coenzyme CoQ10 has been helpful in some patients with MELAS syndrome.
- L-arginine may help to reduce brain damage due to impaired vasodilation in intracerebral arteries owing to nitric oxide depletion
References and Further reading