Learning objectives
- Learning
- Understand
- Integrate
- Reflect
|
Introduction
- Atherosclerosis is a disease of large and medium-sized arteries characterized by endothelial dysfunction, vascular inflammation and accumulation of lipids, cholesterol, calcium and cellular debris within the intima of the vessel wall [1].
- It is a condition affecting large and medium-sized arteries. It leads to the formation of atherosclerotic plaques which may eventually disrupt the blood flow to target organs either by causing progressive fixed stenosis or by rupture and vessel occlusion.
- It can cause myocardial infarction due to the involvement of coronary arteries, peripheral vascular disease through the involvement of lower limb vessel and renal disease with renal artery stenosis and stroke disease through involvement of aorta and head and neck vessels.

Aetiology
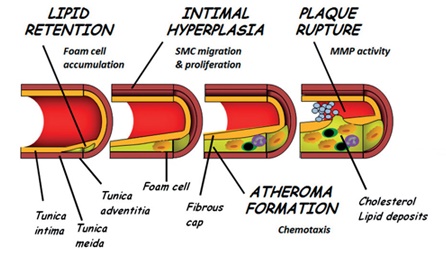
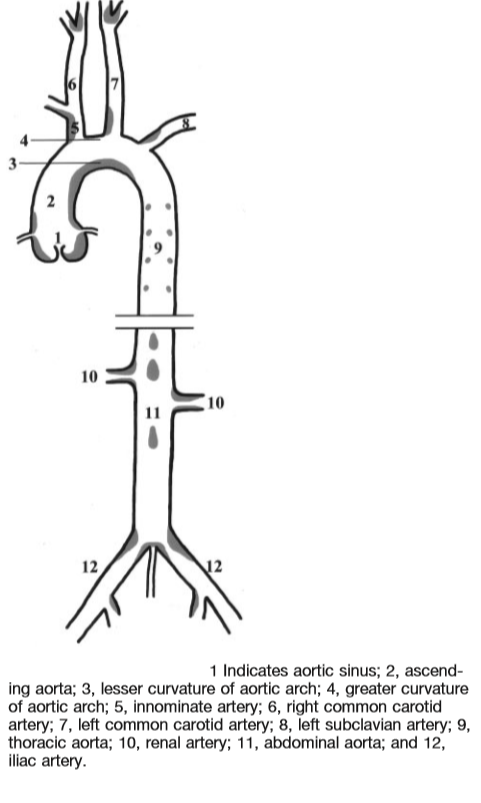
The earliest visible intimal abnormality is a fatty streak seen in the artery and there is entry and accumulation of lipids. Lipids are proinflammatory and cause white cells to accumulate and foam cells (macrophages which release cytokines) formation with intimal damage. This leads to loss of local Nitric oxide vasodilation. Contributing is the fact that smoking causes increased reactive oxygen species (ROS). Over time the overexpression of matrix metalloproteinases [2] breaks down collagen established thinning and weakening of the fibrous cap as the mechanism that renders atheroma prone to rupture. Intimal stable/unstable plaques grow and obstruct the lumen with downstream ischaemia when there is increased O2 demand e.g. exercising causing angina. Intimal unstable plaque can rupture causing the release of thrombogenic material with in-situ thrombosis and vessel occlusion. Intimal unstable plaque ruptures causing localised thrombosis which then embolise downstream. Biomarkers of Atherosclerotic Plaque Instability and Rupture can be detected[3]. Atherosclerosis appears to localise to certain areas on the vascular tree which are associated with regions of low shear stress, oscillatory flow, or turbulent flow. These regions of disturbed flow are related to the anatomy of the vascular tree and are found in areas of branching or high vessel curvature. This can be shown in the diagram below.
Epidemiology
Atherosclerosis remains a major contributor to morbidity and mortality in the Western World. Many risk factors, such as hypercholesterolemia, modified lipoproteins, hypertension, diabetes, infections and smoking have been identified in the development of atherosclerosis.
Carotid Plaque

Infographics
Risks
| Risk factors |
|---|
| Dyslipidaemia (elevated LDL, decreased HDL) | Excess LDL accumulates in the intima and undergoes modifications that initiate and perpetuate the development of atherosclerotic lesions. HDL does not accumulate in vessel walls can even move cholesterol out of arterial walls. |
| Tobacco smoking | Enhances oxidative modification of LDL, contributes to endothelial dysfunction via oxidant stress and increases expression of leukocyte adhesion molecules, among other factors |
| Hypertension | Increases permeability of vessel wall to lipoproteins. Promotes retention of LDL in the vessel intima by increased production of LDL-binding proteoglycans by Smooth muscle cells |
| Diabetes mellitus | Enhances glycation of LDL and is associated with endothelial dysfunction |
| Obesity and lack of physical activity | Contribute to dyslipidaemia, hypertension and insulin resistance |
| Non-modifiable risk factors |
|---|
| Advanced age | Age is a strong risk factor |
| Male gender | Lack of atheroprotective properties of oestrogen which raises HDL and lowers LDL
|
| Heredity | history of coronary artery disease (CAD) among first-degree relatives at a young age (before 55 for males and before 65 for females)
|
| Biological markers |
|---|
| Homocysteine | High levels may promote oxidative stress, vascular inflammation and platelet adhesiveness |
| Lipoprotein particle Lp(a) | Detrimental effect may be attributed to competition with normal plasminogen activity |
| C-reactive protein and other markers of inflammation | Activates complement and contributes to a sustained inflammatory st |
Clinical
- Angina: chest pain with exertion due to a partially blocked coronary artery
- Myocardial infarction: heart muscle damage due to a vessel total or subtotal occlusion and usually causes severe chest pain
- Arrhythmias and sudden cardiac death
- Ischaemic stroke or TIA due to disease of extracranial vessel subclavian, carotids, vertebral
- Ischaemic stroke or TIA due to disease of intracranial carotid, MCA, ACA, PCA, Basilar and circle of Willis
- Peripheral vascular disease with limb claudication or acute ischaemia
- Renal disease due to atherosclerotic renal artery stenosis
Investigations
- FBC, U&E, Glucose, LFTS, Lipids, TFT, CRP
- ECG, CXR
- CT +/- CTA head for acute stroke
- USS Duplex of carotid for stenosis
- Coronary angiography for Acute STEMI
- Troponin for chest pain
Differentials
- Takayasu's arteritis affecting large arteries of the aortic arch
- Carotid dissection causing vessel narrowing or obstruction
Management
- ABC as needed. Cardiac cases need a CCU bed and early access to defibrillation
- In acute STEMI then PCI is needed. Medical care for stable NSTEMI. Antiplatelets are started acutely in Acute MI
- Ischaemic stroke consider reperfusion therapies with thrombectomy/thrombolysis in Stroke.
- Initial rest. HASU for stroke. CCU for MI.
- Immediate Smoking cessation
- Commencement of high dose statin
- Diabetes and BP control
- Long term weight reduction, exercise etc.
References