Learning objectives
|
Histologically the cerebral cortex is made up of a half centimetres of grey cells above a dense thick inner layer of white matter. The overall surface area is increased by the folds of sulci and gyri. The cortex can be seen to be composed of six layers of cells which vary in size and structure. Back in 1909 Brodmann produced a map of the cerebral cortex based on the micro-architecture of the cells and staining for Nissl substance which separates neurons from glial cells. This was before we had understanding of many of the functions of these areas and the system has stood the test of time. Other improvements have been developed by others. It is quite clear that anatomy is related to function.
Cells in the cortex are arranged in a columnar structure and can this can be seen with microelectrode stimulation. Areas with similar function lie close together. For example Broca's area lies within the inferior region of the precentral motor cortex near to those areas that control voluntary movement of the lips, tongue, larynx and pharynx. Broca's produces the content of speech content and damage here leads to an expressive dysphasia. A lesion in the inferior area of the precentral motor cortex leads to dysarthria and facial weakness. Broca's discovery of dysphasia in a patient whose subsequent post mortem revealed a lesion due to syphilis in the area that became known as Broca's area was one of the key finding to suggest localization of function within the brain. The fibres from the cortex on their way to the brainstem pass down in a fan like bundle called the corona radiata to enter the internal capsule.
Note that neuroanatomical diagrams are ?upside down' compared with the normal appearance of imaging
The Cerebral cortex is the most developed part of the human brain and often quoted as the most complicated system and poorly understood system known. The surface is the processing centre comprised of the outer layer of grey matter formed by neuronal cell bodies and their many connections. These are connected with neighbouring areas by axonal extensions which are myelinated and pass to other cortical areas or down and medially as long tracts to brainstem and spinal cord whereas others form circuits within the deep grey matter of the basal ganglia and other structure grey matter structures such as the thalamus or pass to other areas on the cortex. These fibres contain ascending (mainly sensory) and descending signals (mainly motor). The hemispheres surround the fluid filled ventricles.
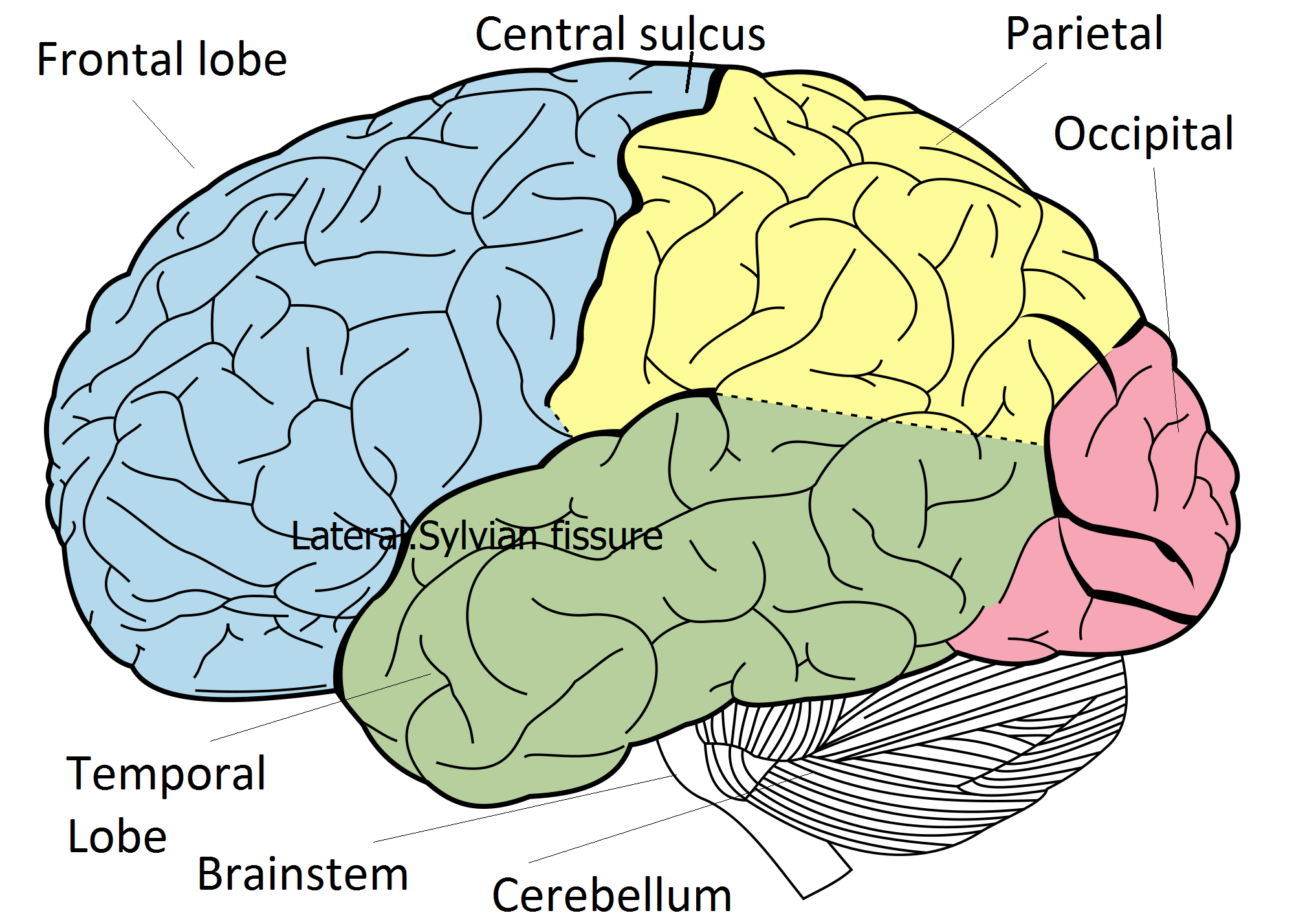
The cerebral hemispheres can be divided by certain sulci on the brain surface into lobes. The surface shows multiple folds - gyri and sulci which increase the amount of grey matter and cortical neurons (processing potential) making up the surface of the brain. It was Broca who showed that different parts of the brain had distinct functions in a patient with a syphilitic lesion in the precentral gyrus and dysphasia. Later others such as Brodmann mapped these areas on their cellular appearance. Let us look at the histology and then the lobes and their function.
The Cerebral cortex is the most developed part of the human brain and often quoted as the most complicated system and poorly understood system known. The surface is the processing centre comprised of the outer layer of grey matter formed by neuronal cell bodies and their many connections. These are connected with neighbouring areas by axonal extensions which are myelinated and pass to other cortical areas or down and medially as long tracts going to brainstem and spinal cord whereas others form circuits within the deep grey matter of the basal ganglia and other structure grey matter structures such as the thalamus or pass to other areas on the cortex. The hemispheres also contain fluid filled ventricles. The cerebral hemispheres can be divided by certain sulci on the brain surface into lobes and the folds increase the amount of grey matter making the surface of the brain. It was Broca who was one of the first to show that different parts of the brain had distinct functions. Others such as Brodmann mapped these areas. Let us look at the histology and then the lobes and their function.
Histologically the cerebral cortex is made up of a 5mm layer of grey cells above a dense thick inner layer of white matter. The overall surface area is increased by the folds of sulci and gyri. The cortex can be seen to be composed of six layers of cells which vary in size and structure. Back in 1909 Brodmann produced a map of the cerebral cortex based on the micro-architecture of the cells and staining for Nissl substance which separates neurons from glial cells. This was before we had understanding of many of the functions of these areas and the system has stood the test of time. Other improvements have been developed by others. It is quite clear that anatomy is related to function.
Cells in the cortex are arranged in a columnar structure and can this can be seen with microelectrode stimulation. Areas with similar function lie close together. For example Broca's area lies within the inferior region of the precentral motor cortex near to those areas that control voluntary movement of the lips, tongue, larynx and pharynx. Broca's produces the content of speech content and damage here leads to an expressive dysphasia. A lesion in the inferior area of the precentral motor cortex leads to dysarthria and facial weakness. Broca's discovery of dysphasia in a patient whose subsequent post mortem revealed a lesion due to syphilis in the area that became known as Broca's area was one of the key finding to suggest localization of function within the brain. The fibres from the cortex on their way to the brainstem pass down in a fan like bundle called the corona radiata to enter the internal capsule.
The Cerebral cortex is the most developed part of the human brain and often quoted as the most complicated system and poorly understood system known. The surface is the processing centre comprised of the outer layer of grey matter formed by neuronal cell bodies and their many connections. These are connected with neighbouring areas by axonal extensions which are myelinated and pass to other cortical areas or down and medially as long tracts to brainstem and spinal cord whereas others form circuits within the deep grey matter of the basal ganglia and other structure grey matter structures such as the thalamus or pass to other areas on the cortex. These fibres contain ascending (mainly sensory) and descending signals (mainly motor). The hemispheres surround the fluid filled ventricles.
The cerebral hemispheres can be divided by certain sulci on the brain surface into lobes. The surface shows multiple folds - gyri and sulci which increase the amount of grey matter and cortical neurons (processing potential) making up the surface of the brain. It was Broca who showed that different parts of the brain had distinct functions in a patient with a syphilitic lesion in the precentral gyrus and dysphasia. Later others such as Brodmann mapped these areas on their cellular appearance. Let us look at the histology and then the lobes and their function. Important surface sulci to identify
For the stroke physician you need to appreciate these anatomical markers on imaging so that you can name the borders of the lobes of the brain on axial, coronal and sagittal planes.
Frontal lobe
The frontal lobe starts at the central sulcus and forwards. Inferiorly limited by the lateral (sylvian) sulcus. The primary motor cortex (MC) lies on the prefrontal gyrus. Input is received from the thalamus and cerebellum and is the main source of all conscious movement. Representation on the lateral surface is hand superiorly and then below that face and tongue and larynx and pharynx. The trunk and leg are represented on the medial inner surface. The Premotor cortex (PMC) lies slightly anterior to MC and is also concerned with voluntary movement. Frontal eye fields lies in front of the PMC and is involved in eye movement. Broca's area (dominant hemisphere) lies inferiorly close to the primary motor areas for mouth, oral cavity and pharynx and larynx. Broca's is involved in generating the content of speech. Damage here causes expressive dysphasia. The Frontal association cortex gets input from thalamus, limbic system, other cortical areas and is involved in intellectual ability. The paracentral lobule found on the medial surface involved with urinary continence.
Parietal lobe The parietal lobe lies behind the central sulcus as far back as the limit of the sylvian (lateral) sulcus and the parietooccipital sulcus. It contains the Primary sensory cortex with representation of hand and face laterally and leg on the inner superior medial section. Areas of high sensory input such as face and hand are given proportionally large representations. All conscious sensation is perceived here. Parietal association cortex mostly involved with integration of sensory input and processing. Input mainly from the thalamus. Deep fibres carry the optic radiations from lateral geniculate ganglion from the superior retina Temporal lobe Temporal lobe lies below the sylvian (lateral) fissure as far back as a line dropped from the end of the sylvian fissure. Contains the Auditory cortex lies in the superior temporal gyrus on lateral surface and is concerned with input from medial geniculate body. Temporal association cortex integrates auditory stimulus and language comprehension (dominant hemisphere) Damage here can cause a receptive dysphasia. Memory processing and recall. Deep fibres carry the optic radiations from the lateral geniculate body from the lower retina
Occipital lobe Occipital lobe lies behind the parietal and temporal lobes. Calcarine cortex primarily deals with vision and visual processing. The optic radiations pass back from the lateral geniculate body of the ipsilateral thalamus. Sight from the right side of ones world goes to left occipital cortex. Occipital association areas concerned with image processing. High density of neurons. The main centre for processing is within the calcarine sulcus. Upper fibres from the upper retina pass to the upper calcarine sulcus called the cuneus. Lower fibres pass to the lower part of the sulcus, the lingual gyrus from the lower retina. The visual area is called Brodmann 17 area.
Insular cortex
This area of grey matter is seen if one parts the lips of the lateral sulcus and is known as the insula. It is closely associated with the middle cerebral artery which passes on the surface. Its functions are poorly understood and possibly involve belching, salivation, gastric movements, and vomiting. It may play a role in addiction. The insula certainly is discussed in early stroke imaging 'loss of the insular ribbon sign'.
Embryologically the eye is an outgrowth from the diencephalon. The Optic nerve is formed at the rear pole of the eye exiting medially at the blind spot. It is not a peripheral nerve but a nerve tract and myelinated by oligodendrocytes rather than Schwann cells. As such it is not vulnerable to peripheral demyelinating neuropathies but can be affected by central demyelinating diseases eg MS. It leaves the orbit through the optic canal passing medially. At the optic chiasma the nasal retinal fibres cross over and temporal retinal fibres stay on the outside. Fibres cross over at the optic chiasma above the pituitary fossa. The tract passes back send most fibres to the lateral geniculate body as well as ipsilateral pretectal nuclei and superior colliculus. On leaving the lateral geniculate body the tract splits into two tracts with an inferior "Meyer's loop" which passes forwards before radiating posteriorly through the temporal lobe along the inferior horn of the lateral ventricle and then to the lower bank of the calcarine sulcus of the occipital cortex and carries information from the inferior retina. The other fibres loop back more directly through the parietal lobe through the retrolenticular part of the internal capsule before passing on to the occipital lobe particularly the upper bank of the calcarine sulcus.
A large venous structure carrying blood from the face indeed the most complex venous plexus in the body. Receives blood from inferior and superior ophthalmic veins and anterior temporal veins and drains into the superior and inferior petrosal sinuses. Pathology includes thrombosis which may be due to localised infection or a prothrombotic disorder or a caroticocavernous fistula with pulsatile exophthalmos. It is also a site for meningiomas. Contents
This is a right-angled shaped tract which carries various ascending and descending myelinated fibres from the cerebral cortex to the thalamus, brain stem and cerebellum as well as basal ganglia structures. It is sandwiched between the structures of the basal ganglia which is a collection of neuronal cell bodies involved in motor function. Contains a high density of ascending and descending tracts fibres. Small ischaemic lesions or bleeds can cause significant deficits. The volume of damage in the primary motor cortex to give a weak arm and face would be much greater than a small lesion in the posterior limb of the internal capsule. Anatomically it can be said to have four parts. On a horizontal section or axial view on MRI it can be seen to have an almost half X shape.
Vascular supply to the internal capsule is by small right angled penetrating arteries of the MCA called the lateral striate (lenticulostriate) arteries and the more anterior aspects including anterior limb by branches of the anterior choroidal artery (a branch of the ICA). The basal ganglia is a collection of interconnected nuclei (neuronal cell bodies) lying deep below the cortex. It is composed of the following structures. The putamen (laterally) and globus pallidus (medially) form the lenticular or lentiform nucleus (lens shaped). The caudate and putamen are also called the neostriatum. Grey matter strands cross the internal capsule to connect these structures and so gives the area the name of the corpus striatum. The putamen is the larger ovoid mass which lies laterally with its lateral side separated very slightly from insular cortex and the external capsule and claustrum. Medially attached to the Globus Pallidus. The Globus Pallidus is smaller triangular shaped structure and lies medially with its medial relation being the internal capsule. The globus pallidus is a major source of output from the basal ganglia. It is divided by a lamina into Globus pallidus externa and interna.
The caudate nucleus is a large mass of grey cells making up a head, body and tail. Anteriorly seen on scans at the lateral border of the anterior horn of the lateral ventricle. It lies then on the lateral wall of the ventricle and there is a tail which passes to form the roof of the inferior temporal horn of the ventricle. The internal capsule separates it from the putamen. The caudate is notable as being diminished in size in Huntington's chorea. The caudate and putamen receive stimulatory input from the cerebral cortex mediated (Glutamate) and from the substantia nigra (Dopamine). The caudate/putamen gives inhibitory output (GABA) to the Globus pallidus and substantia nigra. The Globus pallidus and Substantia nigra also send inhibitory signals to the ventral thalamic nucleus of the thalamus (GABA) which in turn feeds to the cortex (glutamate). The Basal ganglia is concerned with movements of the contralateral limbs and it would seem that it stimulates and inhibits various regions thus modulating motor output. All of these structures are prone to lacunar infarcts and deep haemorrhage

Cerebral Architecture
Lobar Anatomy
Lobar Anatomy

Visual Pathway
Cavernous sinus
Internal Capsule
Basal ganglia