Learning objectives
- Learning
- Understand
- Integrate
- Reflect
|
Introduction
- It was first described as a distinctive syndrome by Hinchey in 1996.
- Sporadic disease seen in children and adults.
- There is posterior circulation vasogenic oedema on MRI which resolves
Aetiology
- Increased vessel permeability and break down in blood-brain barrier
- Vasogenic oedema may be seen on CT/MRI
- Hypertension and failure to autoregulate
- Hormonal changes, Toxic exposure to drugs
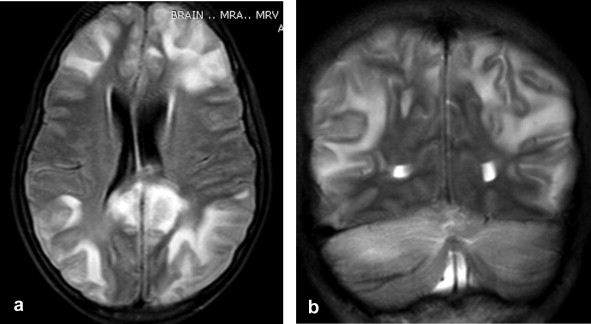
Imaging
| A trigger is usually identifiable, most commonly, acute hypertension (AKI or eclampsia or illicit drugs) or the other group are due to Sepsis and multi-organ failure and Autoimmune disease |
Clinical
- Acute encephalopathy, headache and visual loss
- Dominant finding is seizures (90%) which are usually tonic-clonic. Status epilepticus.
- Visual impairment due to occipital lobe involvement includes hemianopia and visual hallucinations and visual neglect
- Dull bilateral headache and confusion and lethargy
- Symptoms come on over 12-48 hours and resolve within a week, sometimes a little longer.
- Hypertension is common but may be secondary to PRES rather than a cause.
Investigations
- Bloods: There may be an increase in LDH, reduced platelets, Low Mg, Raised LDH
- CT: is only helpful in half the cases.
- MRI: diagnosis is confirmed on MRI scan with the presence of bilateral vasogenic oedema with hyperintensities on FLAIR predominantly in the parietal/occipital region but sometimes in frontal lobes, temporooccipital and cerebellum [Barynski WS 2008].Extensive lesions on T2 weighted imaging tend to have a worse prognosis [Covarrubias DJ et al. 2002]. The lesions are due to vasogenic oedema and there is not usually restricted diffusion but in some cases DWI changes with restricted diffusion are seen. All of these changes should resolve with time.
- Angiography: Angiography in PRES demonstrates reversible focal and diffuse abnormalities and vasoconstriction, vasospasm (diffuse or focal)
- EEG is non-specific with diffuse slowing or focal δ waves.
Causes or Triggers of PRES
| Causes or Triggers of PRES with Comments |
|---|
| Preeclampsia/eclampsia | No difference in out come than with non pregnant PRES. Give IV Magnesium, Caesarean section |
| Renal failure | Manage as usual |
| Severe Hypertension | Keep BP below 160 mmHg and avoid nitroglycerin |
| Ciclosporin/Tacrolimus and others | Within 2 weeks of drug starting. management is to withdraw therapy |
| Post Transplantation | Within first month post transplantation |
| Autoimmune | SLE, WG, SS, PAN |
| Infection | Treat Sepsis syndrome. Abnormal LFTs, Renal function, Multiorgan failure. |
| Neuromyelitis optica | suggests a defect in free water movement [Magana SM et al. 2009] |
Differentials
- Bilateral PCA infarcts
- Venous sinus thrombosis or subdural, intracerebral, or subarachnoid haemorrhage can all present with headache, seizures, reduced consciousness, and focal neurologic signs but Non contrast CT is diagnostic
- Infective encephalitis or meningitis, particularly herpes simplex encephalitis (Figure 3), should be considered, and rapid treatment with IV Aciclovir and antibiotics may be lifesaving while a diagnosis is still being pursued.
- Basilar artery thrombosis can present with progressive neurologic deficits and can result in tetra paresis, coma, or locked-in syndrome.
- Central nervous system vasculitis can mimic PRES but the MRI findings are usually more diffuse and irreversible.
Management
- ABC, Supportive, Manage BP and treat any specific cause
- As the name implies there is reversibility. Haemorrhage is possible.
- Recovery usually happens over several weeks. Repeat MRI after 10 days should show improvement.
- Blood pressure may be a primary or secondary phenomenon but BP control is advocated but not with nitro-glycerine due to negative reports.
- Seizures seem to burn out and so long-term AEDs not needed.
- Recovery is the rule and outcomes excellent but this ultimate prognosis depends on the underlying cause.
Reviews and references