Learning objectives
- Learning
- Understand
- Integrate
- Reflect
|
Introduction
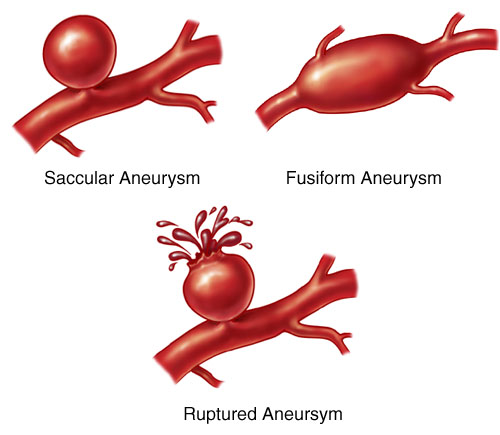
Saccular (Berry) aneurysms are developmental abnormalities in the blood vessel of the circle of Willis and their branches. They may be due to an inherited connective tissue weakness, anatomical defects and abnormal flow patterns. They are not detectable at birth or in childhood but then appear in early adult life and begin to enlarge and become more detectable in later life. They can remain silent lifelong or in some patients can bleed and cause subarachnoid haemorrhage (5% of all strokes). They can enlarge and cause local pressure effects e.g. IIIrd nerve palsy. They are found in 1-2% of the population which in the UK suggests 0.6-1.2 million individuals. Only a minority present with an acute bleed and 90% are less than 10 mm diameter. 15% have multiple aneurysms. The risk of rupture of an asymptomatic intracranial aneurysm is approximately 0.7%. This discussion should also be read with the article on Subarachnoid Haemorrhage. Berry aneurysms are the commonest but not the only cause of SAH.
Images
Presentation
- Thunderclap headache and/or collapse due to acute bleed from aneurysm into subarachnoid space. Needs fast track to neurosurgeon for immediate management.
- Saccular aneurysms are the most important cause of primary non-traumatic SAH and account for 70-80% of all SAH.
- Asymptomatic aneurysm picked up on imaging for some other reasons or screening of 1st degree relatives.
- Pressure symptoms as the aneurysm enlarges. Giant aneurysms can be defined as those over 25 mm and within the skull the pressure effects maybe significant.
- Ipsilateral IIIrd nerve: Posterior communicating artery or Superior Cerebellar artery Aneurysm
- Brainstem signs mainly hemiparesis as a basilar artery aneurysm compresses ventrally
- Ophthalmic artery aneurysm causing retro-orbital pain
- Middle cerebral artery aneurysm: Hemiparesis or aphasia
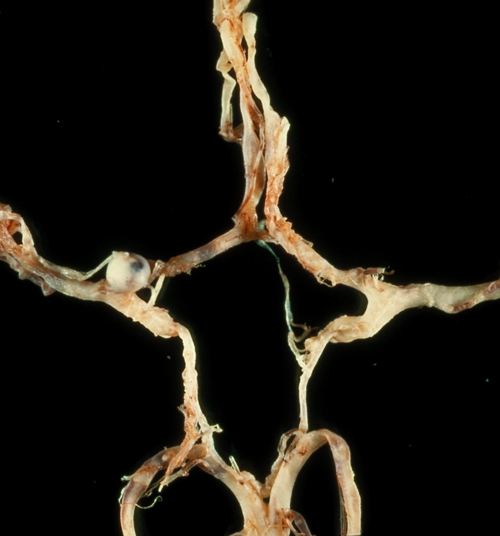
Anatomy
- Anatomically aneurysms have a neck and a dome or fundus and this can be assessed radiographically.
- They tend to form at the site of arterial bifurcations.
- The aneurysmal pouch is composed of thickened hyalinised intima with the muscular wall and internal elastic lamina being absent as the normal muscularis and elastic lamina terminate at the neck of an aneurysm.
- If an aneurysm grows it can become irregular in outline and may have mural thrombus and become paper thin. Rupture occurs from the dome.
Risks
- Ageing, smoking and hypertension.
- Risks to suggest rupture are increasing size, prior SAH from another aneurysm, cigarette smoking, location in the basilar apex and posterior communicating artery aneurysm.
Associations
- Ehlers-Danlos syndrome (type IV), Marfan syndrome
- Autosomal dominant polycystic kidney disease (ADPKD)
- Coarctation of aorta, bicuspid aortic valve
- Neurofibromatosis type 1 (NF1)
- Hereditary haemorrhagic telangiectasia
- Alpha 1 antitrypsin deficiency
- Cerebral AVM
- Fibromuscular dysplasia
- Thoracic and abdominal aortic aneurysms
Sites
| Anterior Circulation | Posterior Circulation |
|---|
- 90% Anterior circulation. 20% have multiple aneurysms
- ACA/ACoA complex: 30-40%
- Supraclinoid ICA and ICA/PCoA junction: ~30%
- MCA (M1/M2 junction) bi/trifurcation: 20-30%
|
- 10% Posterior circulation
- Basilar tip
- Superior cerebellar artery
- Posterior inferior cerebellar artery
|
Imaging Berry Aneurysms
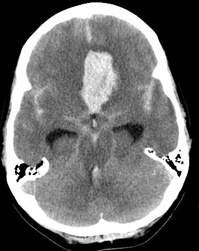
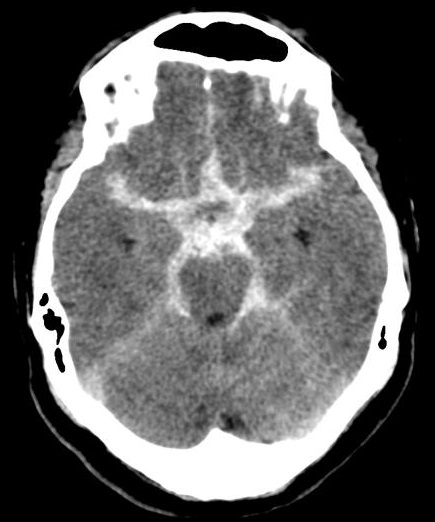
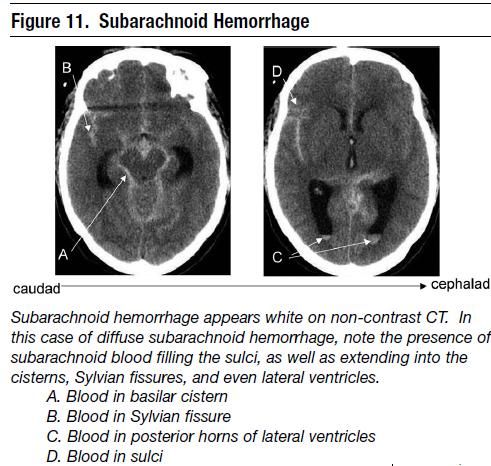
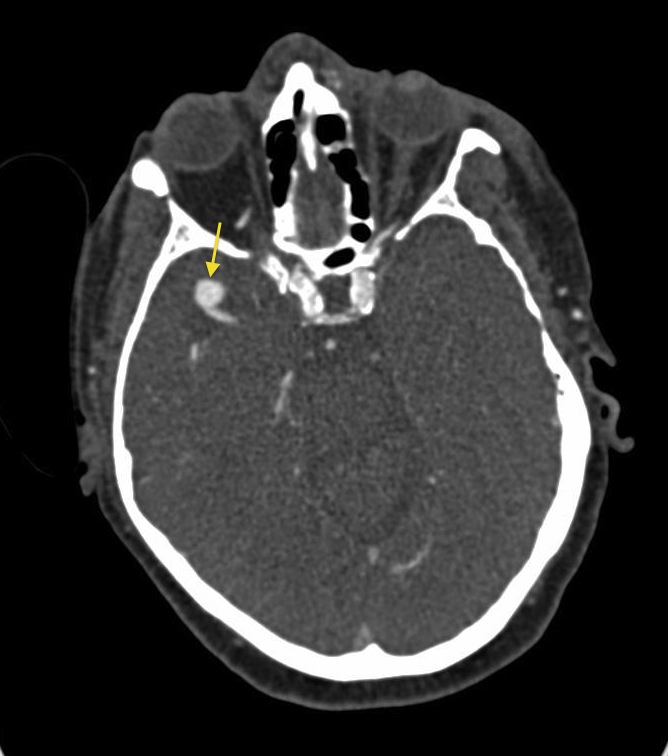
- Non-Contrast CT: In acute SAH blood may be seen within the subarachnoid space or can by intraparencymal depending on the position of the aneurysm. The aneurysm may be detected simply due to the location of the densest collection of blood and an outline of aneurysm may be seen. In that situation if possible, a CTA should be done.
- CT angiography (CTA): Appearance depends upon the presence of thrombosis within an aneurysm. Aneurysm appears as a well-defined round, slightly hyperattenuating lesions. Calcification can be present. Post contrast? Patent aneurysm: bright and uniform enhancement. Thrombosed aneurysm: rim enhancement due to filling defect
- MR angiography (MRA): On MRI also the patent and thrombosed aneurysm display different imaging features: On T1 most of the patent aneurysm appears as a flow void, or they may show heterogeneous signal intensity in thrombosed aneurysm appearance depends on the age of clot within the lumen. On T2 typically hypointense laminated thrombus may show a hyperintense rim
- Digital subtraction (catheter) angiography (DSA): tends to exist in tertiary centres where there is intention for active management and is considered the gold standard in most institutions. It has been reported more sensitivity in 3D DSA over 2D DSA when regarding the detection of small aneurysms. Attention must be given when measuring the aneurysm neck size as it can be overestimated by the 3D reconstructions.
Treatment and prognosis
Treatment of large or symptomatic aneurysms should be considered, with either endovascular coiling or surgical clipping. Management of small aneurysms is controversial. Those less than 7 mm in maximal diameter artery low risk and unlikely to rupture but there are statistically more of these so there are the rare cases of patients with small aneurysms which have ruptured resulting in subarachnoid haemorrhage, often with devastating consequences.
|
Five-Year Cumulative Percentage Risk of Rupture of Previously Unruptured Aneurysms According to the ISUIA Study |
| Aneurysm Size vs. Localisation | <7 mm* | 7-12 mm | 13-24 mm | >24 mm |
| Intracavernous ICA | 0 | 0 | 3.0% | 6.4% |
| Other ICA, MCA, ACA | 0 (1.5%) | 2.6% | 14.5% | 40.0% |
| Posterior circulation and posterior communicating artery | 2.5% (3.4%) | 14.5% | 18.4% | 50.0% |
- Clipping: Neurosurgical aneurysm clipping requires a craniotomy, performed under general anaesthesia. It takes 4-8 hours and has a procedural mortality rate of 1-3%. Early clipping - less rebleeding but higher incidence of vasospasm. Worst time is day 7 to 10 (highest time for vasospasm) So < 3 days or > 10 days. Notably Coils are not MRI compatible and is avoided. CT will also show lots of artefact.
- Coiling: Endovascular obliteration by means of platinum spirals (coiling) is the preferred mode of treatment. It is a minimally invasive percutaneous endovascular treatment, which has proved to be a safe alternative to traditional surgical clipping of the aneurysm and may be associated with a better outcome in selected patients. The technique consists of packing the aneurysm with detachable coils and is performed under general anaesthesia. It avoids craniotomy, and recovery after the procedure is more rapid. It is not indicated in 5-15% of cases, due to morphological or positional aneurysm characteristics. Performed by neurosurgeon or interventional neuroradiologist. Notably Coils are usually MRI compatible. CT will show lots of artefact, so MRI preferred.
- Clipping vs Coiling: International Subarachnoid Aneurysm Trial (ISAT) Lancet 2002. 2143 patients randomized to NS clipping (n=1070) or endovascular coiling
(n=1073). Outcomes at 2 months and 1 year. Better outcome with coiling with 23.7% vs 30.6% dependent or dead at 1y (ARR 7% NNT 14)
| Clipping requires craniotomy | Coiling can be done by catheter |
|---|
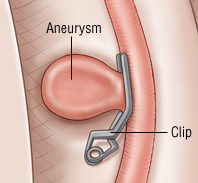 | 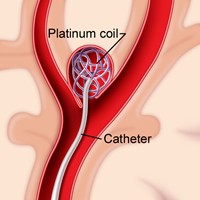 |
Other Aneurysms
Fusiform Aneurysms
- Elongated spindle shaped aneurysms due to atherosclerosis and ectasia of large arteries.
- As they enlarge they may compress surrounding structures with focal neurological results, e.g. as facial pain (Trigeminal), hemifacial spasm (Facial), and hearing loss with vertigo (VIII).
- They rarely rupture; but if they do, total occlusion is usually required because their stiff walls and shape make surgical clipping difficult.
Mycotic Aneurysms
- Most commonly related to endocarditis as an infected embolism enters distal branch of a cerebral artery to cause a microinfarction or micro abscesses.
- The artery can rupture, or arteritis or mycotic aneurysms develop which later rupture.
- Treatment is to treat the endocarditis. Intervention is unusual. Anticoagulation can cause bleeding.
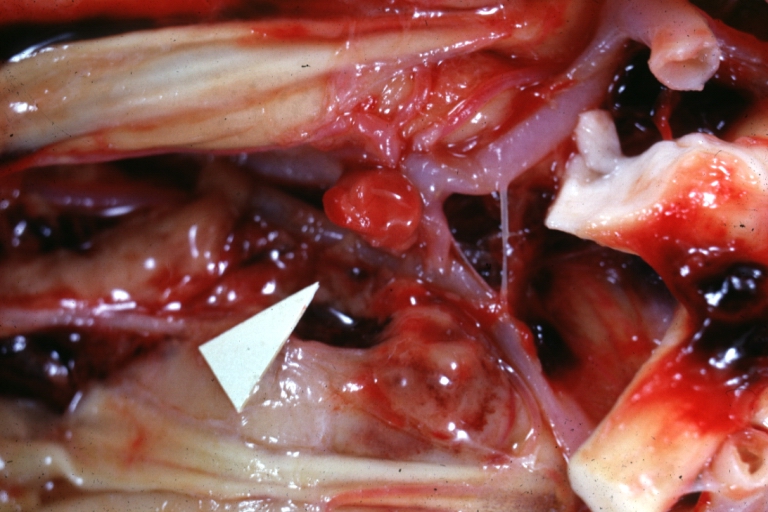
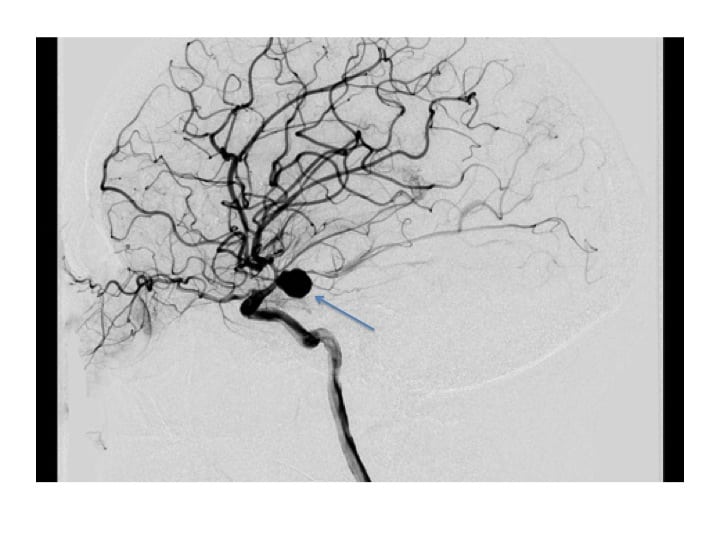 Pcomm aneurysm
Pcomm aneurysm