Learning objectives
|
Introduction
- Infarction or haemorrhage into the spinal cord is by definition a strokes
- Spinal strokes are rare and make up 1% of known strokes
- Presentation is with a spinal cord syndrome that needs differentiation from other causes
- The ability to improve is much reduced compared with the brain
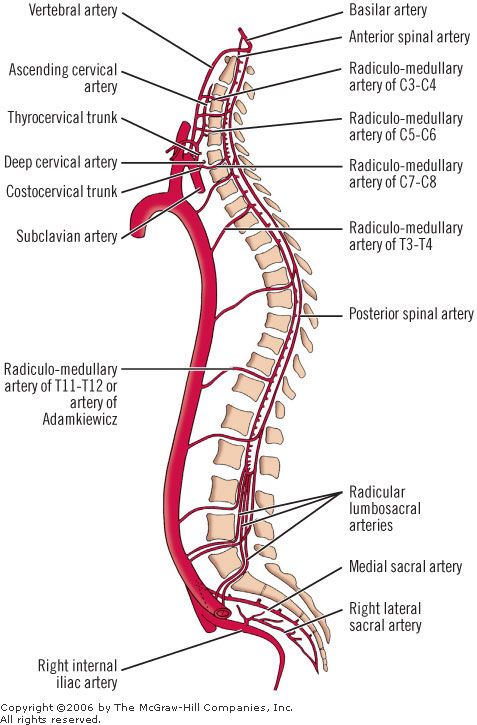
Anatomy
Vertebral arteries are the main source of blood to the spine which are the
- One anterior spinal artery : which runs along the anterior median fissure and supplies the anterior grey column, lateral grey column, central grey matter (lamina X), anterior funiculus (white matter), lateral funiculus the anterior portion of the posterior grey matter. Three quarters of the blood supply to the cord are derived from the anterior spinal artery.
- Two posterior spinal arteries : which run (one on each side of the midline) along the posterolateral sulcus (i.e., along the line of attachment of the dorsal nerve roots). These supply the posterior grey column (including lamina I – VI) and posterior funiculus
| The blood supply of the spinal cord is poorest between levels T4 and T9 |
Aetiology
- The anterior spinal artery comes off the Aorta and can be affected by emboli, aortic surgery or drops in BP
- Thoracoabdominal aortic repair operations e.g. Type B Aortic dissections
- Haemorrhagic cord disease associated with spinal AVMs, coagulopathies dealt with elsewhere
- Venous infarction due to dural arteriovenous malformation
Epidemiology
- They account for 1.25% of all strokes.
Risk factors
- Atherosclerosis, Thoracoabdominal aortic disease
- Atrial fibrillation, Vasculitis
- Smoking, diabetes, syphilis, hypertension
Clinical
- Weakness, sensory symptoms, bladder and bowel incontinence
- Spastic Weakness both legs (paraparesis)or both arms and legs (quadriparesis)
- Loss of pain and temperature sensation below level
- Preservation of dorsal column function - light touch and vibration and proprioception
- Often comes on acutely and may be seen post op AAA repair
- May have embolic disease e.g. AF, peripheral vascular disease
Investigations
- Standard stroke bloods - exclude vasculitis
- ECG and/or 24 hr tape
- Echocardiogram
- Thrombophilia screen
- CT of thorax and abdomen to rule out aortic dissection
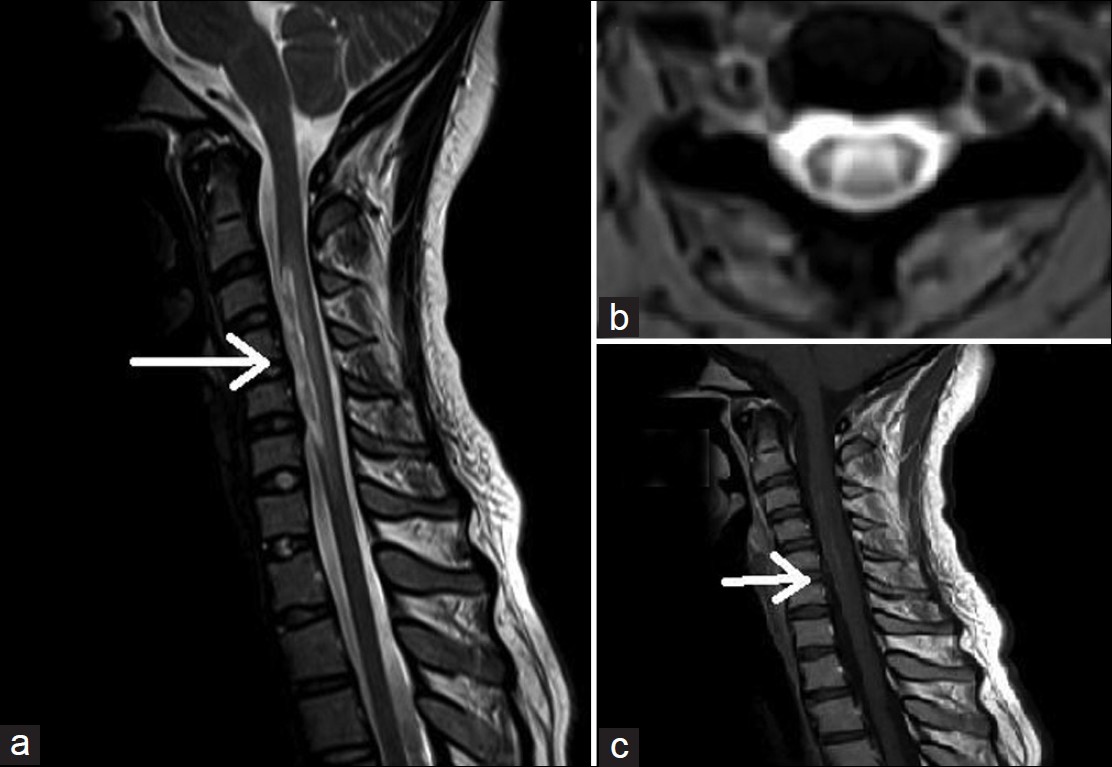
- MRI may show restricted diffusion on multiple levels
- MR angiogram is a useful tool for screening AVM in suspected spinal strokes.
Differentials
- Transverse Myelitis due to Demyelination: MS, ADEM, NMO
- Tumour
- Infections causing Transverse Myelitis
Complications
- Paraplegia, Incontinence
- Venous thromboembolism, Sepsis
- Sexual dysfunction
- Muscle/joint pain and neuralgia
- Anxiety, depression
Management
- Acutely ABC. IV steroids may be given.
- A lumbar drain may be placed to drain cerebrospinal fluid (CSF) in anticipation of possible further cord swelling and oedema.
- Keep mean arterial pressure (MAP) goals adjusted to at least >70 mmHg (ideally >80 mmHg) to increase perfusion to the spinal cord.
- Follow local protocols. Often not managed on stroke unit but may go to spinal centres
- Antiplatelets, anticoagulation as needed. Statins
References
Last updated: 18/11/2018
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |