Learning objectives
|
MRI Basics
Unlike CT, which requires ionising radiation, MRI is based on the interaction between radio waves and hydrogen nuclei in the body in the presence of a strong magnetic field. There is no ionising radiation and no known safety issues. MRI produces higher quality images than CT. In CT scans must be in the plane of the gantry, that is, axial or semi-coronal. In MRI, one is able to acquire images directly in any plane, that is, the usual axial, sagittal, coronal, or any other.
Both modalities focus on the properties of a volume element or "voxel" of tissue. This is represented in 2-D form or picture elements or "pixels". The pixel intensity in CT reflects the electron density but in MRI it reflects the density of hydrogen, generally as water (H20) or fat. To be more exact, MR signal intensity reflects the density of mobile hydrogen nuclei modified by the chemical environment, that is, by the magnetic relaxation times, T1 and T2, and by motion.
A hydrogen nucleus is a single proton. It has a positive charge and spins and so generates a small magnetic field (a "magnetic moment") which are usually randomly distributed. These magnetic moments align when placed in a larger magnetic field. With MRI the magnetic field across the body-sized sample is intentionally made non-uniform by superimposing additional magnetic field gradients that can be turned on and off rapidly. Activation of these additional magnetic fields results in a net gradient in the strength of the magnetic field across the body which is necessary for spatial localisation and imaging. The essential components of an MR imaging system include a large magnet which generates a uniform magnetic field, smaller electromagnetic coils to generate magnetic field gradients for imaging and a radio transmitter and receiver and its associated transmitting and receiving antennae or coils. In addition to these fundamental components, a computer is necessary to coordinate signal generation and acquisition and image formation and display.
When the body lies within a strong magnetic field, it becomes temporarily magnetised. This state is achieved when the hydrogen nuclei in the body align with the magnetic field. When magnetised, the body responds to exposure to radiowaves at a particular frequency by sending back a radiowave signal called a "spin echo". This phenomenon (NMR) only occurs at one frequency (the "Larmor frequency") corresponding to the specific strength of the magnetic field. The spin echo signal is composed of multiple frequencies, reflecting different positions along the magnetic field gradient. When the signal is broken into its component frequencies (by a technique called a "Fourier Transform"), the magnitude of the signal at each frequency is proportional to the hydrogen density at that location, thus allowing an image to be constructed. Thus, spatial information in MRI is contained in the frequency of the signal, unlike X-ray-based imaging modalities such as CT.
Sometimes MRI is not possible
Brain MRI usually involves lying within a very tight space for between 10 and 30 minutes. Access to the patient is difficult. It is incredibly noisy and communication with radiographers is difficult. One has to be realistic and consider the shortest protocol that will get the important clinical information needed. Some do not tolerate it at all. It is a common paradox and frustration that those in whom it would be of most value can't have one due to one reason or other. There are some open scanners available for those who are claustrophic but access is often difficult.
| Reasons why MRI not possible |
|---|
|
Examples
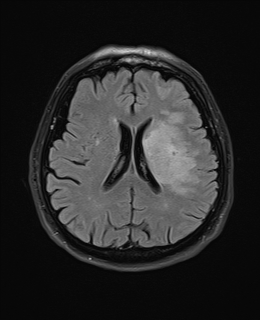
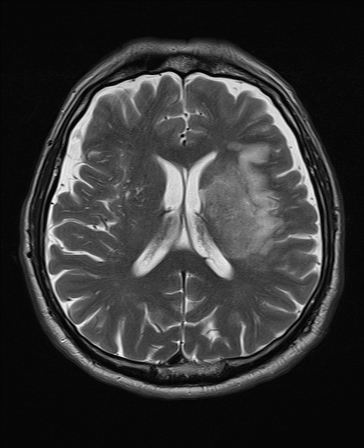
| T2 FLAIR | T2 |
|---|---|
 | 
|
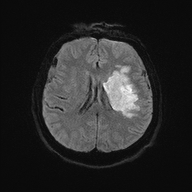
| DWI | ADC |
 | 
|
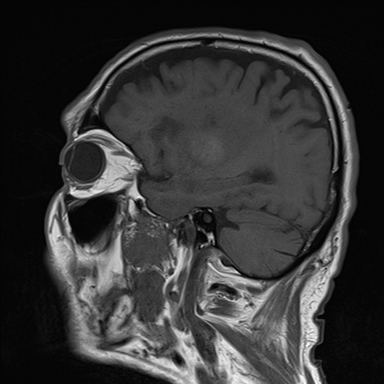
| SWI | T1 Sagittal |
 | 
|
Metal outside the brain and eye is NOT an absolute contraindication: Magnetic deflection is minimal compared to normal physiologic forces. Cardiac valves), inferior vena cava filters, biliary and vascular stents, IUD's and metallic prostheses are safe, unless there is doubt as to positional stability. MRI Policies - Safety and Contraindications . Information is changing all the time. Another useful site is MRI safety.com
MRI with Gadolinium
This is the MRI equivalent of CT with contrast and uses Gadolinium which shortens T1 relaxation times. It is useful when there is suspicion of neoplastic, inflammatory lesions or abscesses. Also useful for detecting meningeal disease. It is not often used in acute stroke unless the diagnosis is in doubt.
MR Angiography
Scan Sequences
Relaxation times
- T1 relaxation time: Time taken for 63% of longitudinal magnetisation to recover in a tissue. T1 is short in fat and long in water and proteins. Contrast causes T1 shortening.
- T2 relaxation time: Time taken for 63% of transverse magnetisation to be lost in a tissue. Liquids have long T2 and large molecules a short T2.
- T2* based on T2 decay and dephasing due to inhomogeneities in the magnetic field. Relevant in Gradient echo imaging.
- Weighting T1 and T2 weighting can increase tissue contrast
T1 weighted
- Scanning parameters are set (short TR/short TE)
- Dark : CSF and anything with increased water (oedema, tumour, infection, infraction, haemorrhage or flow void or calcification).
- Bright: Fat, subacute haemorrhage, melanin, protein rich fluid, slow flowing blood, gadolinium, laminar necrosis of an infarct. White matter is brighter than grey. Myelin is light grey. Grey matter is grey. T1 is better for showing anatomy. An acute stroke will be hypointense.
T2 Weighted
- Dark: Calcification, Blood products, protein rich fluid, flow void.
- Bright: Anything with increased water e.g. CSF, Oedema, tumour, Infarct, inflammation, infection, subdural collection, methaemoglobin in subacute bleed. CSF is white and brain tissue is darker and more intermediate. Fat is dark. Myelin is dark grey. Grey matter is brighter than white matter. Good for identifying pathology. T2 is bright due to water or any oedema in pathology. For example a fresh infarct with oedema will show up bright or hyperintense after a few days becoming most obvious after a few months. T2 weighted hyperintensities may be seen within 6 hours and are present in 90% by 24 hours.
T2* "star"
- T2* can be recorded using GRE sequences with a low flip angle, long TE, and long TR
- Mostly used to detect iron in its various forms. Haemorrhages cause an influx of hemoglobin and hemosiderin into the lesion.
- The iron in haemoglobin and haemosiderin is paramagnetic and thus causes an susceptibility difference in the damaged region, which shows up as dark regions in T2* scans.
- Blood looks black and Hemosiderosis can also be detected by T2* scans for the same reason.
- Calcification shows up bright in a T2* MRI due to its higher diamagnetism than the surrounding tissue.
FLAIR
- Fluid attenuated inverse recovery.
- FLAIR scans are T2 scans with the free water signal nulled.
- CSF is now dark. Useful to see oedema and periventricular lesions which appear bright.
- An acute ischaemic stroke will be bright
Gradient echo (GRE)
- Excellent at identifying areas of blood and haemosiderin deposition such as in macrophages around an old bleed.
- Also useful in identifying microbleeds. Sensitivity for blood approaches CT within first 24 hours of a bleed.
- After several days GRE is the more sensitive modality.
Diffusion Weighted Imaging
- Identifies areas where Brownian motion is restricted due to cytotoxic cell death. Useful for identifying early Ischaemic stroke.
- This is explained by loss of ATP causes of ion exchange pumps.
- Water from the extracellular space enters into the intracellular compartment (cytotoxic oedema) and produces a typical bright spot on DWI.
- These changes are seen even within 30 minutes. A new stroke is bright but an old stroke will have low signal intensity on DWI.
- The DWI is initially bright white and then gradually fades after 10-15 days when the lesion will be best seen on T2 and FLAIR.
- The ADC often shows the inverse and is black.
- The signal intensity of acute stroke on DW images increases during the 1st week after symptom onset and decreases thereafter.
- The ADC map shows a similar findings.
| Restricted diffusion: Bright DWI and Dark ADC |
|---|
|
| Left MCA infarct | DWI of an Anterior cerebral artery infarct |
|---|---|
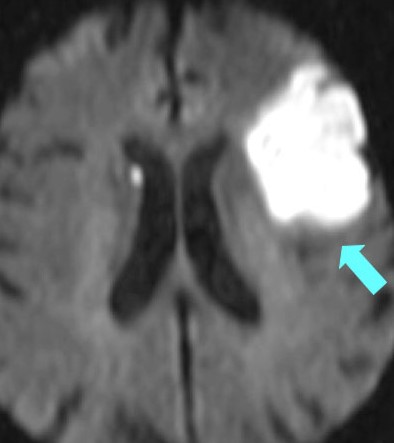 | 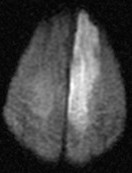 |
Apparent Diffusion Coefficient: (ADC map)
Used with DWI. Ischaemic lesions appear dark.If bright this may suggests the DWI increased signal changes are due to T2 shine through and old i.e. false positive.
Gadolinium Enhancement
Identifies pathology in which there is breakdown of the blood brain barrier. Also useful in producing an angiogram. Tumours or other lesions may show ring like enhancement. T1 with Gadolinium will show increased signal with a pituitary tumour, acoustic neuroma or meningioma.
Susceptibility weighted imaging (SWI)
SWI is an MRI sequence sensitive to paramagnetic compounds which distort the local magnetic field. It can detect blood, iron and calcium etc. and so is useful to detect haemorrhage or blood. Images generate a unique contrast, different from that of spin density, T1, T2, and T2*. It is very sensitive over other sequences. It is not possible to differentiate calcium from blood. A filtered phase can allow distinguish between the two as diamagnetic and paramagnetic compounds will affect phase differently (i.e. veins / haemorrhage and calcification will appear of opposite signal intensity). SWI is very useful in detecting cerebral microbleeds in ageing and occult low-flow vascular malformations, in characterising brain tumours and degenerative diseases of the brain, and in recognizing calcifications in various pathological conditions. The phase images are especially useful in differentiating between paramagnetic susceptibility effects of blood and diamagnetic effects of calcium. SWI can also be used to evaluate changes in iron content in different neurodegenerative disorders. Reference

MRI Imaging
| Acute Ischaemic Stroke |
|
| Cardioembolic stroke |
|
| Lacunar Stroke |
|
| Basilar Artery Occlusion |
|
| Carotid Dissection |
|
| Cerebral/Vertebral venous sinus thrombosis |
|
| CADASIL |
|
| Primary angiitis of the CNS |
|
| MELAS syndrome |
|
| Posterior reversible encephalopathy syndrome (PRES) |
|
Imaging Patterns in Haemorrhagic Stroke
| Hypertensive haemorrhage |
|
| Cerebral Amyloid Angiopathy |
|
Other relevant imaging Diagnoses
Non Communicating Hydrocephalus
Radiology of choice is Midsagittal MRI which reveals the drainage pathway in great detail
- Normal - Lateral ventricles small and 3rd ventricle barely visible
- Single lateral ventricle dilated (Univentricular hydrocephalus) = Obstruction of one foramen of munro
- Both lateral ventricles dilated (Biventricular) = Obstruction of both foramen of munro
- Dilation of Lateral + 3rd Ventricle (Triventricular) = Obstruction at level of aqueduct
- Dilation of Lateral + 3rd + 4th = Obstruction at foramen of Magendie and Luschka
Communicating Hydrocephalus
- All ventricles are modestly dilated.
- Prominent Subarachnoid spaces and basal cisterns
Last updated: 18/11/2018
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |