Learning objectives
- Understand the aetiology and risk factors for lacunar strokes
- Be able to recognise the clinical presentation
- Discuss diagnostics and treatment strategies
Historical aspects
- The concept of lacunar stroke was first described by Dechambre in the early 1800s
- Lacunes were small cavities found at post mortem
- Further clinical correlation by Charles Miller Fisher in the 1960s who recorded about 15 clinical types
| Lacunar strokes are probably part of the spectrum of small vessel disease (SVD), which affects small arteries, arterioles, venules, and capillaries in the brain, has long been associated with cognitive impairment and dementia<. Lacunes are Predictors of Cognitive Decline in Cerebral Small-Vessel Disease |
Introduction
- Lacunar strokes make up about 20% to 30% of all Ischaemic strokes
- Short term their prognosis is good but long term they suggest increased risk of death and cognitive decline.
- Lacunes involve small branches of the larger arteries < 0.4 mm in diameter and are usually end arteries with no collaterals.
- These are branches of arteries 4-8 mm in diameter which is a 10 fold drop in size/diameter.
- The gradual reduction in calibre is not seen so these small vessels are more vulnerable to elevated blood pressure.
- Lacunae, or small-vessel strokes, large overlap with small vessel disease but SVD is the pathology and lacunar strokes the effect.
- The ostia of the penetrating vessels may be occluded by a large thrombus within the lumen of the main vessel.
- The strokes in this case are usually larger than a single lacune and would not represent true penetrating artery disease.
Vessels and Site
- Lenticulostriate (MCA)
- Anterior striate
- Heubner arteries
- Thalamoperforators (PCA)
- Deep perforators of basilar
- Deep cerebral white matter
- Basal ganglia,
- Basic pontis (pans) due to occlusion of a single small perforating artery supplying the subcortical areas of the brain.
Aetiology
- Hypertension documented in 90% of those with Lacunar strokes though this has been questioned in other studies
- Commoner in African Caribbean origin, diabetes and hypertension
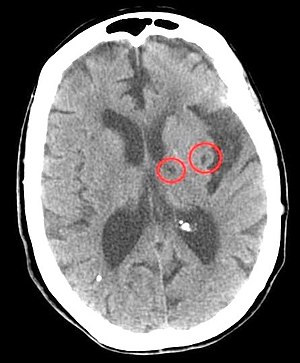
- Acute lesions well seen on MRI and sometimes CT
- Rounded infarct cavities with a diameter < 1.5 cm are found
- Small vessels exposed to high blood pressures
- Occluded by lipohyalinosis/fibrinoid necrosis or microemboli
- Microatheroma and Arteriolosclerosis related to vascular risk factors
- The areas typified by lacunar infarcts also are the setting of hypertensive bleeds
- It is also the area most affected by microbleeds which may leave behind small cavities
Anatomy of lesions
- Centrum semiovale, Caudate nucleus, internal capsule
- Globus pallidus and Putamen and Thalamus
- Brainstem and Cerebellum midline
- Rounded infarcts with a diameter < 1.5 cm
- Small vessels exposed to high blood pressures
Risk Factors
- 90% have a history of Hypertension
- Commoner in African Caribbean origin
- Diabetes, Smokers
Vessels affected
- Medial/Lateral Lenticulostriate branches of ACA/MCA
- Thalamogeniculate/perforant branches of PCA
- Paramedian branches of Basilar artery

Clinical lacunar syndromes
Lacunar strokes are typically subcortical involving white matter tracts and so classically no cognitive loss, aphasia or other higher functions affected. May at times be a staggered slow presentation.
| Syndrome | Clinical correlation |
|---|---|
| Pure Motor Stroke (PMS) | Usually the commonest in clinical practice. Unilateral, pure motor deficit. Clearly involving two of three areas (face, arm and leg) With the whole of any limb being involved. Can be anywhere along the corticospinal tract including the posterior limb of the internal capsule or the basis pontis. |
| Pure Sensory Stroke (PSS) | Unilateral purely sensory symptoms ( +/- signs) Clearly involving two of three areas (face, arm, and leg) With the whole of any limb being involved. Lesion in the brainstem or thalamus (ventral) or thalamocortical projections classically. |
| Ataxic Hemiparesis (AH) | Ipsilateral cerebellar and corticospinal tract signs . With or without dysarthria . No higher cerebral dysfunction or a visual field defect. Lesion can be anterior limb of internal capsule or corona radiata. Others report posterior limb IC, thalamus, lentiform nucleus and cerebellum. |
| Sensorimotor Stroke (SMS) | PMS and PSS combined (i.e., unilateral motor and sensory signs and symptoms) . No higher cerebral dysfunction or a visual field deficit. Lesion in thalamus/internal capsule or corona radiata |
| Dysarthria-clumsy hand syndrome | dysarthria and upper limb ataxia and clumsy hand. Usually a lacune of the anterior limb of the IC. Also in pontine lesions |
| Basilar branch syndromes | |
| Silent | a great number of lacunes cause no symptoms at all and are only found incidentally on imaging. In fact silent are 5 times as common as non silent. |
Differential
- Striatocapsular infarcts: embolic occlusion of the MCA often occludes penetrating branches and results in subcortical infarction which can resemble a lacunar but is usually larger and more crescentic in shape.
- Microbleeds : these form in the same areas. They can leave behind small cavities. My need Gradient echo and similar protocols to try and identify causality.
- Vascular spaces: may be seen in the subcortical areas. Not pathological.
Investigations
- FBC, U&E, LFTs, ESR
- ECG : LVH changes
- CT: can only pick up lesions > 2 mm. Lacunar infarcts appear as rounded lesions in classical penetrating artery distributions usually < 15 mm in diameter in brainstem, thalamus, internal capsule
- MRI:more sensitive especially for lesions in pons. Restricted diffusion and reduced ADC for acute lesions. For older lesions the question is are these ischaemic or haemorrhagic cavities. Gradient echo and similar protocols can help define these.
- Angiography: may suggest that small vessels occluded due to large vessel disease or occlusion e.g. a non occlusive thrombus in Basilar artery.
- Screening for CADASIL if appropriate
Management
- There is a clear link with Hypertension so this is the main focus with aggressive lifetime lowering of BP to < 140/90 mmHg as well
- Management of coexisting diabetes, lipids, smoking cessation.
- Consider antiplatelets, statins though the evidence base is not as strong as with other ischaemic stroke causes.
References
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |