Learning objectives
|
Introduction
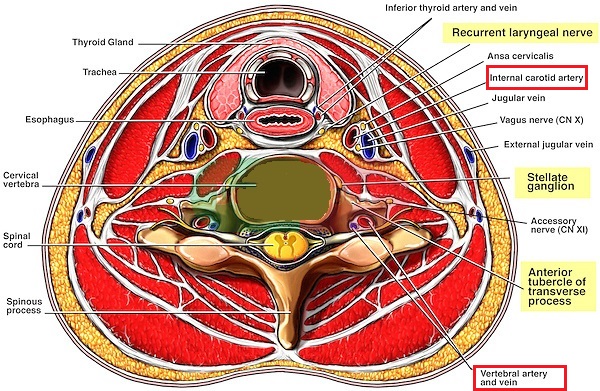
Any cross section through the mid neck has 4 arteries that supply the brain. These are the right and left internal carotid arteries and the right and left vertebral arteries. The area of the brain supplied by the internal carotid is called the anterior circulation and that supplied by the vertebral/basilar artery the Posterior circulation. It is from this that we get the Oxford stroke classifications e.g. TACS vs POCS as these vessels are associated with specific clinical syndromes.
This is important as these vessels may be the source of or the route of emboli to the brain. The vessels themselves may block and cause stroke. These vessels are the route by which interventional neuroradiologists get access to the large vessels and to the circle of Willis.
Cross section of Neck showing relative positional anatomy of Carotid and vertebral and other neck structures
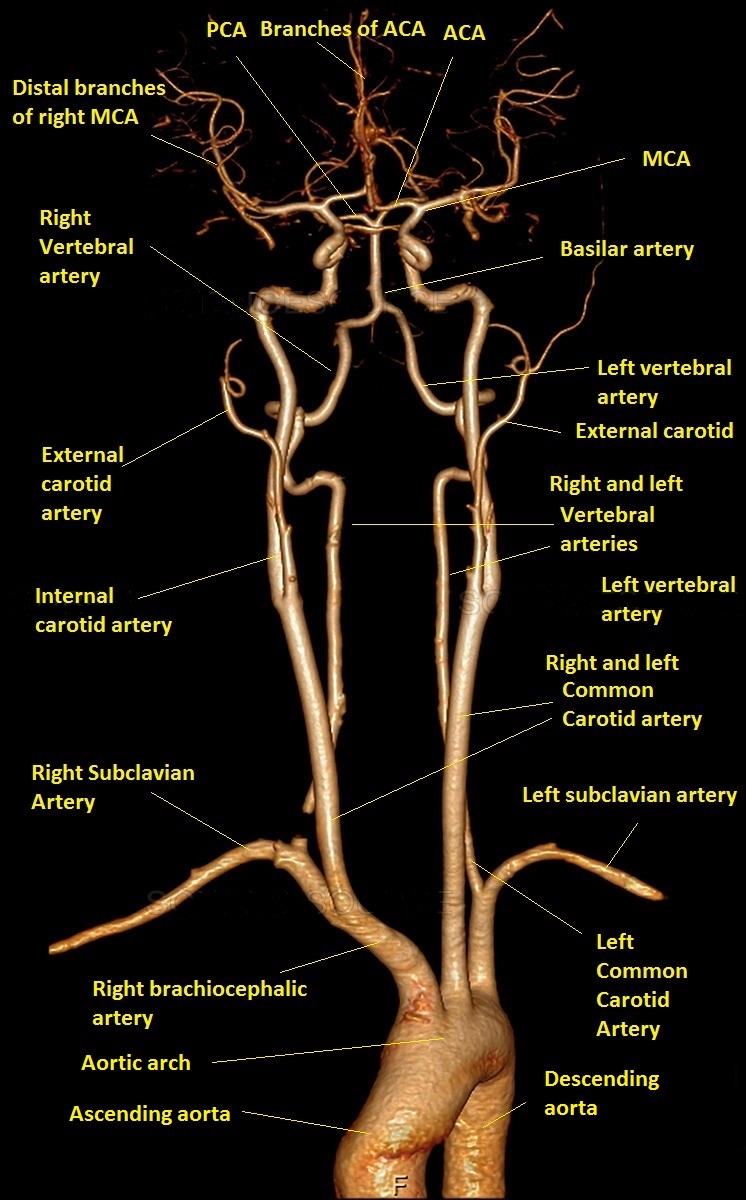
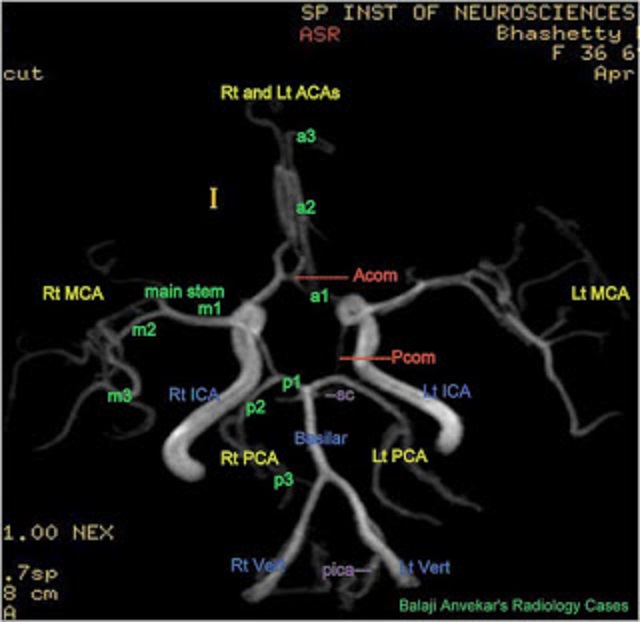
Angiogram of the head and neck vessels from Arch to Cerebral vertex
It is important to quickly get used to the appearance of angiography and the normal anatomy of both carotids and vertebral arteries which are quite distinctive. The easiest thing to spot is the fusion of the vertebrals into the basilar artery and the very tortuous sigmoidal bends of the carotid artery. Once you can identify each major vessel then it becomes much easier. Almost all arteries are paired with right and left branches except for the basilar artery and the anterior communicating and the artery of percheron. Its a typical rule of thumb that for any other than some rare exceptions the end blood vessels supplying the brain respect and do not cross the midline.
Vascular Anatomy
- Innominate artery
- Right common carotid → Right internal carotid 2/3rds of supply
- Right subclavian artery → Right Vertebral artery 1/3rd of supply
- Left common carotid
- Left internal carotid 2/3rds of supply
- Left external carotid - does not supply brain except through collaterals
- Left subclavian → Left Vertebral artery → Basilar artery → Posterior cerebral artery
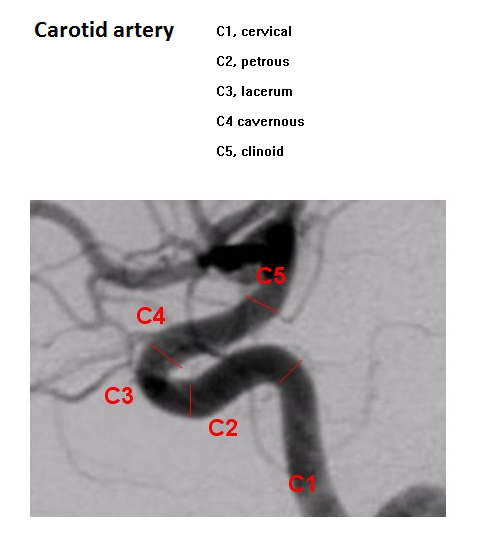
Anterior circulation: Internal Carotid artery
- Cervical segment - within the neck. Associated with sympathetic supply.
- Petrous segment - enters skull via foramen lacerum and runs forwards
- Cavernous segment - enters the cavernous sinus and runs with th VIth nerve and gives off branch superior hypophysial to the posterior pituitary
- Supraclinoid segment - pierces dura and then splits into anterior cerebral artery and middle cerebral artery
- Ophthalmic artery
- First branch of the ICA and enters the orbit with the optic nerve and gives off a branch the central artery to retina. The artery runs forward to supply the eye and scalp around the eye as well as frontal and ethmoidal sinuses.
- Maxillary artery anastomoses provides some collateral flow if proximal occlusion. Occlusion of the ophthalmic artery does not tend to cause blindness and as there are collaterals
- Central artery to the retina: runs along the centre of the optic nerve entering the eye to supply the inner retinal layers. Occlusion will cause monocular blindness
- Posterior ciliary artery is the main source of blood supply to the optic nerve head (ONH), and it also supplies the choroid up to the equator, the retinal pigment epithelium. The blood supply in the ONH is segmental, so that most of its ischemic lesions result in sectoral visual field defects. Vessel involved in Anterior Ischaemic optic neuropathy and Giant cell arteritis.
Posterior communicating artery (PCOMM)
This artery joins the Internal carotid to the Posterior cerebral artery and so joins anterior and posterior circulations. It is closely associated with the IIIrd nerve which can be compressed by an aneurysm of the PCOMM. It irrigates the ventral thalamus, hypothalamus and tail of caudate. In a minority it can be a large "fetal vessel" and in theory can then bring carotid blood into the posterior circulation. In other variants it canbe hypoplastic.
Anterior choroidal artery
This arises from the ICA as can be seen above and Passes posteriorly with branches to supply
- Posterior limb of internal capsule
- choroid plexus of lateral ventricle
- optic tract and lateral geniculate body (hemianopia)
- area of midbrain and globus pallidus and substantia nigra
Anterior cerebral artery
This is a branch of the ICA and lies on the inner medial surface of the cerebrum.It arches up and around and back over the corpus callosum amnd gives off branches
- A1 Segment - from the bifurcation of the internal
carotid to the anterior comm artery. Branches include
- Medial lenticulostriate artery : contributes to anteroinferior part including the anterior limb of internal capsule and anterior portion of caudate and putamen
- Anterior communicating artery connects both ACA and is a common site of aneurysms
- Recurrent artery of Heubner supplies head of caudate and anteroinferior internal capsule
- A2 Pericallosal branch - is the continuation of A1
supplying medial surface of cerebral cortex and corpus callosum after the Anterior communicating branch
- Orbitofrontal
- Polar frontal
- Callosomarginal
Middle cerebral artery
This is formed by the bifurcation of the ICA into MCA and ACA. It passes laterally.
- M1 segment from the bifurcation of the internal carotid
passes laterally to the surface of the insula where it bifurcates.
- Occlusion here may result in massive infarction depending on collateral supply and whether it is proximal or distal to lenticulostriate vessels.
- A clot may be seen in the artery "the hyperdense MCA sign" in which a string of thrombus may be seen within the M1 on Non contrast CT
- Lateral lenticulostriate arteries (Deep penetrating
vessels)
- Branch of at right angles to supply the Globus pallidus and putamen, posterior limb of internal capsule, head and tail of caudate, thalamus and Meyer's loop which includes some of the optic radiations can be caught
- Arterial occlusion typically may cause lacunar type strokes and vulnerable to lipohyalinosis and occlusion
- M2 segment within the sylvian fissure and branch. A
clot here may result in a "dot"sign on CT. The artery branches into
- M3 segments Upper division
- prefrontal (frontal cortex)
- precentral (primary motor and associated areas)
- central (pre/post central gyri)
- post central (primary sensory area)
- parietal (posterior parietal)
- M3 segments Lower division
- middle temporal (mid temporal cortex)
- tempeoroccipitalroccipital (temporal and occipital cortex)
- angular (angular and associated gyri)
- R/L Subclavian artery
- M3 segments Upper division
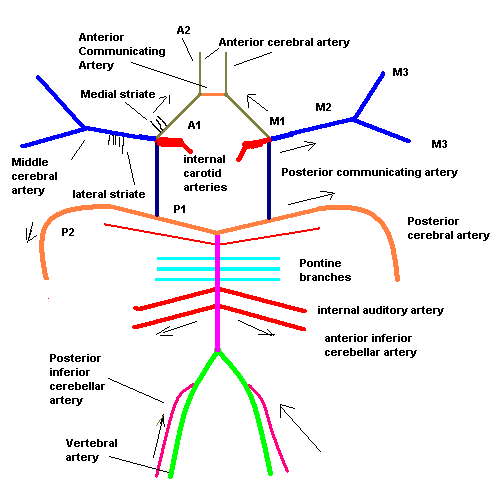
Schematic Diagram of vascular supply
Posterior circulation - Vertebrobasilar system
| Appreciate the path of the artery and the turns it makes before entering the skull The V3 region is the most mobile section and most vulnerable to injury and dissection is possibly commoner here but can happen anywhere along the artery. |
- Vertebral artery - 1st branches of the subclavian
arteries on either side then enter the transverse process at
(C6) and ascends through the foramina in the transverse processes of the upper
six cervical vertebrae to C1 where they enter the foramen magnum in front of
the medulla. Inside the the skull, the two vertebral arteries join to
form the basilar artery.
- Posterior inferior cerebellar artery
- Largest branch of the vertebral and supplies lateral medulla and lateral cerebellum
- Loops around medulla to the inferior surface of cerebellum.
- Occlusion can cause Wallenburg's/Lateral Medullary syndrome
- Infarction of Inferior cerebellum, IX,X,XI, Nucleus ambiguus
- Anterior spinal artery (ventral medulla)
- Forms at the point where the vertebral arteries fuse
- Posterior spinal artery (dorsal medulla)
- Posterior inferior cerebellar artery
- Basilar artery forms at the lower border of the pons by
fusion fo the two vertebral arteries
- Anterior inferior cerebellar artery supplies lateral pons and anteroinferior cerebellum
- Superior cerebellar artery - supplies lateral pons and superior surface of cerebellum
- 12 Pontine arteries penetrate to supply medial pons - are a number of small vessels which come off at right angles from either side of the basilar artery and supply the pons and adjacent parts of the brain
- Internal auditory artery - a long slender branch, arises from near the middle of the artery; it accompanies the acoustic nerve through the internal acoustic meatus, and is distributed to the internal ear
- Posterior cerebral artery (PCA)(embryologically
originate from Internal carotid) passes laterally and is joined by the posterior communicating and then sweeps back around the cerebral peduncle to reach the tentorial surface of the occipital lobe.
- Postero-medial ganglionic branches arise at the commencement of the posterior cerebral artery and with branches from the post comm artery pierce the posterior perforated substance, and supply the medial surfaces of the thalami and the walls of the third ventricle.
- Posterior choroidal branches run forward beneath the splenium of the corpus callosum, and supply the tela choroidea of the third ventricle and the choroid plexus
- Postero-lateral ganglionic branches are small arteries which arise from the posterior cerebral artery after it has turned around the cerebral peduncle; they supply a considerable portion of the thalamus
- Anterior temporal supplies uncus and the anterior part of the fusiform gyrus
- Posterior temporal supplies inferior temporal gyri, calcarine, to the cuneus and gyrus lingualis and the back part of the convex surface of the occipital lobe
- Parietooccipital to the cuneus and the precuneus.
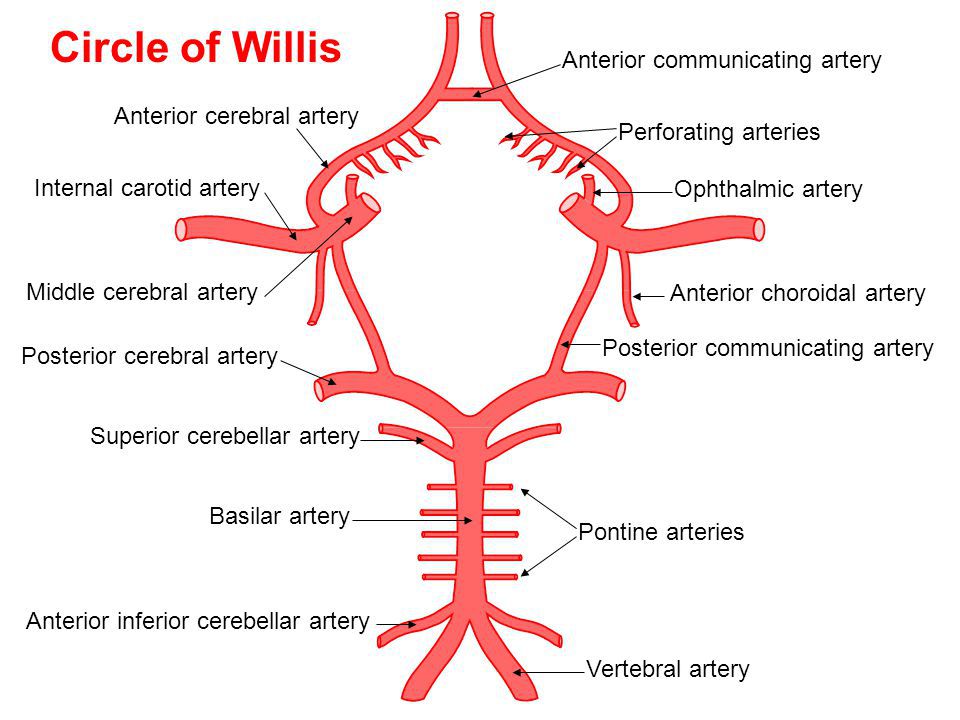
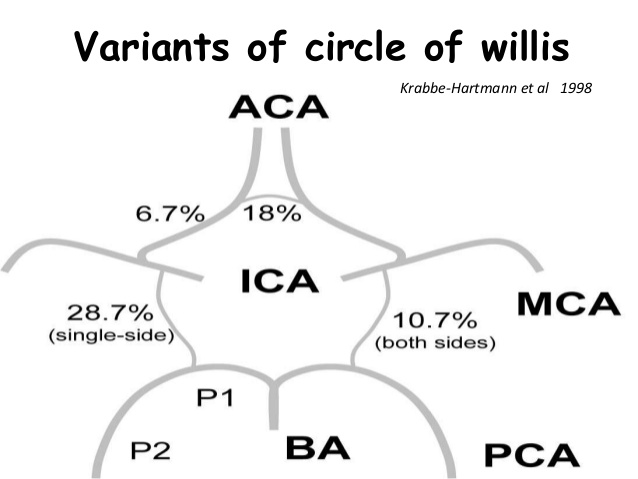
Circle of willis
At the base of the brain lies the COW which is an arterial ring connection beween the posterior communicating vessels which bring the anterior and posterior circulation together and the anterior comunicating circulation which brings togetehr both sides of the anteiror circulation. Some call it a heptagon rather than a circle as it does have seven sides. In about 60% of case the COW is deficient with one or more of the arteries being hypoplastic or even missing. The commonest might be that the A1 segment of ACA is hypoplastic or even absent in 10%, Acom amy be absent in 5% and there may sometimes be an overdevelopped large posterior communicating artery often called a fetal variant which can bring blood from the carotid to the basilar and PCA. This may be seen in 20%. In about a third however the PComm may be small or even absent. Asymmetry and anomalies of the circle of Willis results in significant asymmetry of flow and is an important factor in the development of intracranial aneurysms and atypical ischaemic stroke. Blood in the COW will flow from high to low pressure. There are many variations on the basic layout.
Venous anatomy
- Superior sagittal sinus: Venous blood from the brain passes across the subdural space in the bridging veins and emissary veins into the superior sagittal sinus. The sinus also receives CSF through the arachnoid villi.
- Cavernous sinus: contains various other structures including III, IV and V1, V2 and VI and postganglionic sympathetic fibres and the siphon part of the internal carotid artery
- Great cerebral vein drains deep cerebral structures into the Straight sinus
- Ultimately all venous outflow is to the internal jugular vein


| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |