Learning objectives
- Causes of coma
- Useful signs
- Management of coma
Pathophysiology
- Consciousness is an arousal and awareness of environment and self, achieved through action of the ascending reticular activating system (ARAS) on the brain stem and cerebral cortex [link].
- ARAS is composed of several neuronal circuits connecting the brainstem to the cortex.
- ARAS is composed of structures such as the brainstem nuclei (locus coeruleus, dorsal raphe, median raphe, pedunculopontine nucleus, parabrachial nucleus), and non-specific thalamic nuclei, hypothalamus, and the basal forebrain.
- These structures may come under pressure with subsequent vascular compromise as ICP rises or when bilateral structures are involved such as with bilateral thalamic infarction.
- Compression on brainstem will also lead to damage to the third nerve and dilated pupils with bilateral mydriasis and absence of pupillary light reflex
- Pontine damage however may show small pinpoint pupils.
Raised ICP Causes
- Complete MCA occlusion in young person with small CSF spaces + Malignant MCA
- Acute Carotid T occlusion + Malignant MCA type syndrome
- Extensive ICH
- Above +/- Hydrocephalus
- Space occupying lesion
- Subdural haematoma
- Extradural haematoma
Non Stroke Causes
- Bilateral Thalamic Strokes [link]
- Post Ictal Generalised seizure
- Non convulsive status
- Hypoglycaemia
- Hyponatraemia
- Drugs - opiates etc.
Clinical
- Bilateral Thalamic Strokes [link]
- Generalised seizure
- Hypoglycaemia
- Hyponatraemia
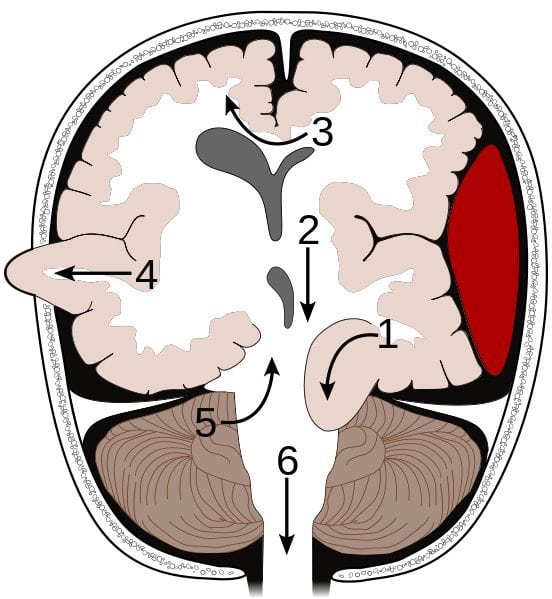
- Supratentorial
- Uncal transtentorial herniation
- Central tentorial herniation
- Subfalcine herniation
- Transcalvarial herniation
- Infratentorial
- Upward transtentorial herniation (“reverse coning”)
- Foraminal or tonsillar herniation (“coning”)
| Herniation | Aetiology | Symptoms |
|---|---|---|
| Foramen magnum | Due to a posterior fossa SOL or from further progression of a supratentorial mass lesion or oedema. Compression of cerebellar tonsils and medulla. In the medulla are located the vital centers regulating respiration and cardiac function, and the reticular activating system for maintaining consciousness. | In foramen magnum herniation, the following develop: changes in the level of consciousness, extensor posturing, apnoea, and then circulatory collapse followed by death. |
| Foramen magnum | Due to a posterior fossa SOL or from further progression of a supratentorial mass lesion or oedema. Compression of cerebellar tonsils and medulla. In the medulla are located the vital centers regulating respiration and cardiac function, and the reticular activating system for maintaining consciousness. | In foramen magnum herniation, the following develop: changes in the level of consciousness, extensor posturing, apnea, and then circulatory collapse followed by death. |
Management
- General: ABC, Oxygen, IV fluids. ITU bed if GCS < 9
- Coma cocktail if unsure and no obvious structural cause: Glucose, Naloxone and IV Ceftriaxone and IV Aciclovir
- Raised ICP
- Intubation and ventilation to lower pCO2 to 28-32 mmHg
- Mannitol IV Boluses
- Definitive surgery e.g. Evacuate haematoma, Hemicraniectomy or EVD for Hydrocephalus
- Hypoglycaemia: IV Glucose
- Tumour with oedema: IV Dexamethasone
- Post Ictal: Monitor
- Non-convulsive status: Consider IV Lorazepam
- Bilateral Thalamic Strokes : Supportive care
References
| Note: The plan is to keep the website free through donations and advertisers that do not present any conflicts of interest. I am keen to advertise courses and conferences. If you have found the site useful or have any constructive comments please write to me at drokane (at) gmail.com. I keep a list of patrons to whom I am indebted who have contributed. If you would like to advertise a course or conference then please contact me directly for costs and to discuss a sponsored link from this site. |